- Visibility 74 Views
- Downloads 7 Downloads
- DOI 10.18231/2456-9267.2019.0011
-
CrossMark

Classification of breast lumps on the basis of fine needle aspiration cytology or FNAC
Abstract
Introduction: FNAC is an essential part of the triple assessment method of preoperative evaluation of breast lumps or masses. So the aim of our present study is evaluation of the accuracy and effectiveness of FNAC for classification of breast lumps in our institute.
Materials and Methods: The present retrospective study was conducted at the Department of Pathology, GMERS Medical College & Hospital-Junagadh (Gujarat, India) from January 2017 to December 2018. Specific inclusion and exclusion criteria were used in order to select the cases for the present study. Necessary and relevant data was statistically evaluated in terms of sensitivity, specificity, PPV, NPV, FPR, FNR and overall diagnostic accuracy. Kappa statistics and Chi-square tests were applied for further statistical significance.
Results: Out of 215 cases of breast lumps that underwent FNAC, a total number of 145 cases were evaluated and classified into five categories from unsatisfactory (C1) to Malignant (C5). Sensitivity, specificity, PPV, NPV, FPR, FNR and overall diagnostic accuracy were 90.90%, 98.68%, 1.37%, 9.09%, 96.77%, 96.15% & 96.33% respectively.
Conclusion: On the basis of FNAC reports, we can classify breast lesions into various categories from C1 to C5 and these cytological categories show a statistically significant correlation with final diagnoses given in subsequent histopathology reports.
Keywords: Breast lumps, Classification, Benign, Malignant.
Introduction
A palpable Lump or Mass is the commonest mode of presentation of various diseases of the breast and preoperative evaluation remains always essential as a part of their management.[1],[2]This preoperative evaluation or assessment includes combination of clinical assessment, radiological imaging and a tissue sample taken for either cytological or histological analysis, the so-called triple assessment.[3] As a part of this triple assessment, Fine Needle Aspiration Cytology (FNAC) remains always useful and beneficiary for the patients because of a lot of advantages like high accuracy, cheap, fast, out-patient procedure reducing pressure on theatre load, high acceptability, and low complication rate.[4]
According to FNAC reports, breast lumps or masses can be classified into 5 categories based on the National Health Services Breast Screening Programme (NHSBSP) of Britain[5] Such classification becomes helpful in further management of the patient and the diagnostic categories with their corresponding numerical codes are: Inadequate/insufficient (C1); Benign (C2); Atypical/indeterminate (C3); Suspicious of malignancy (C4) and Malignant (C5). The aim of our present study is evaluation of the accuracy and effectiveness of this FNAC based categorization or classification of breast lumps in our institute.
Material and Methods
The present retrospective study was conducted at Department of Pathology, GMERS Medical College & Hospital, Junagadh, Gujarat, India. Duration of the study was two years from January 2017 to December 2018. For statistical analysis, data was collected from cytology & histopathology laboratory registers with some inclusion & exclusion criteria mentioned below:
Inclusion criteria:
- All female patients of different age groups who presented with a palpable breast lump or mass but with unknown primary diagnosis
- Patients who underwent both FNAC at OPD basis & subsequent post-operative histopathological evaluation.
Exclusion criteria:
- Patients who underwent FNAC but did not undergo subsequent histopathological diagnosis.
- Patients with recurrent malignancy.
- Patients with history of past or current chemotherapy or any other forms of treatment.
- Male patients with benign or malignant breast lesions.
Data was evaluated in terms of sensitivity, specificity, positive & negative predictive values, false positive rate, false negative rate and overall diagnostic accuracy. Results were presented in frequency tables & cross tabulations. For statistical evaluation, we utilized the Statistical Package for Social Sciences (SPSS) version 17.0. (SPSS Inc. Released in 2008; SPSS Statistics for Windows, Version 17.0. Chicago, USA).For statistical significance, we utilized the Chi-square (?[2]) test [6] and the Kappa Statistics[7] both.
Result
During last two years (2017 & 2018), a total number of 600 patients were undergone the procedure of FNAC for various lesions & out of them, 215 patients were females who presented with a palpable lump or mass in the breast but having no known primary diagnosis. Left sided lumps or lesions were more common or more in number (60.00%) than right sided ones (40.00%). The commonest location was upper & outer quadrant of breast (49.30%) & next common location was sub-areolar region of breast (16.28%). Less common locations were upper & inner quadrant (16.28%), lower & outer quadrant (11.16%) as well as lower & inner quadrant (6.98%) respectively.
Out of 215 cases, only 145 were undergone subsequent post-operative histopathological evaluation, so we included only these cases for further statistical analysis & evaluation. A total number of 70 patients defaulted from post-operative evaluation because of one reason or another so default rate was 32.56%. Out of 145 cases, 31 were unequivocally malignant (C5) while 78 were benign (C2) i.e. negative for malignant cells. Five cases were benign lesions but having nuclear atypia (C3) while eight cases were suspicious for malignancy (C4). Total 23 FNAC smears were unsatisfactory or inadequate for evaluation (C1) giving unsatisfactory rate of 15.85%.
Age wise distribution of 215 patients, comparative evaluation of cytology reports (categories) of 145 patients and diagnostic validities of FNAC procedure & reports after exclusion of unsatisfactory, atypical & suspicious smears are mentioned below in table no. 1, 2 and 3 respectively.
Table 1: Age wise distribution of patients or cases presented with breast masses (n=215)
|
Age Group in years |
Cytological Category Codes |
Total |
||||
|
C1 |
C2 |
C3 |
C4 |
C5 |
||
|
11-20 |
01 |
26 |
-- |
-- |
-- |
27 |
|
21-30 |
08 |
51 |
-- |
-- |
-- |
59 |
|
31-40 |
09 |
37 |
02 |
-- |
-- |
48 |
|
41-50 |
04 |
27 |
02 |
06 |
13 |
52 |
|
51-60 |
-- |
05 |
01 |
01 |
09 |
16 |
|
61-70 |
01 |
02 |
-- |
01 |
04 |
08 |
|
71-80 |
-- |
-- |
-- |
-- |
05 |
05 |
|
Total |
23 |
148 |
05 |
08 |
31 |
215 |
Table 2: Comparative evaluation of cytology reports (categories) of patients with their subsequent histopathological diagnosis (n=145)
|
|
Histopathological Diagnosis |
|||
|
Cytological Category and Code |
Benign |
Malignant |
Total |
|
|
Insufficient/Unsatisfactory |
C1 |
12 |
11 |
23 |
|
Benign |
C2 |
75 |
03 |
78 |
|
Atypical |
C3 |
03 |
02 |
05 |
|
Suspicious for Malignancy |
C4 |
02 |
06 |
08 |
|
Malignant |
C5 |
01 |
30 |
31 |
|
Total |
93 |
52 |
145 |
|
Table 3: Diagnostic validities of FNAC* procedure & reports after exclusion of unsatisfactory, atypical & suspicious smears (n=109)
|
Diagnostic Validity |
Formula |
Value in Percentage |
|
Sensitivity |
TP/(TP+FN) |
90.90 |
|
Specificity |
TN/(FP+TN) |
98.68 |
|
False Positive Rate |
FP/(FP+TN) |
1.37 |
|
False Negative Rate |
FN/(FN+TP) |
9.09 |
|
Positive Predictive Value (PPV) |
TP/(TP+FP) |
96.77 |
|
Negative Predictive Value (NPV) |
TN/(TN+FN) |
96.15 |
|
Overall Diagnostic Accuracy |
TP+TN/(TP+TN+FP+FN) |
96.33 |
|
*FNAC = Fine Needle Aspiration Cytology, TP = True Positive, FP = False Positive TN = True Negative, FN = False Negative |
||
Results mentioned above, show a significant correlation between cytology & histopathology reports in cases of both benign (C2) & malignant (C5) breast lesions. Concordance rates for both benign (C2) & malignant (C5) categories are 96.15% and 96.77% respectively. Kappa value (?) for C2 or benign category is 0.912. SE (?) is 0.043 & 95% confidence interval is 0.828-0.996. These statistical values show almost perfect agreement between cytology & histopathology
reports for benign lesions. Similar results are obtained for C5 or malignant category also. Total (?[2]) value for both categories is 90.766 & corrected (?[2]) value (after Yate’s correction) is 86.402. These both values are quite higher with Probability value (P) of less than 0.001. Both Kappa (?) as well as Chi-square (?[2]) tests show statistically significant relationship between cytology & histopathology reports in case of both benign & malignant lesions.
 |
Click here to view |
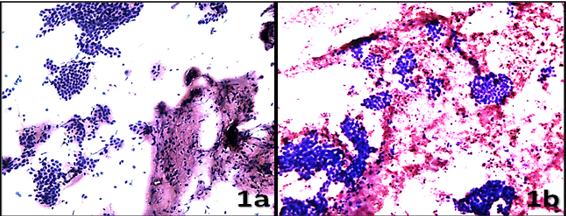
Fig. 1: Cytomorphology of benign breast lesions (H & E, 100x), 1a] benign, proliferative & typical appearance (C2) and [1b] benign lesion with nuclear atypia (C3)
 |
Click here to view |
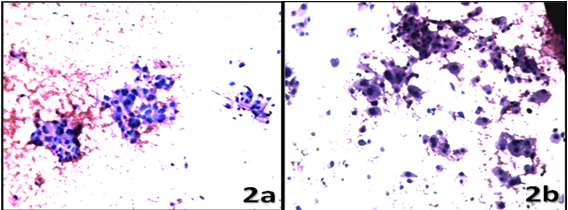
Fig. 2: Cytomorphology of malignant breast lesions (H & E, 100x), 2a] cells are cohesive and having mild to moderate anisonucleosis (suspicious for malignancy or C4) and 2b] quite dis-cohesive cells with marked anisonucleosis leading to diagnosis of malignancy (C5)
Fig. 1 shows cytomorphological features of benign breast lesions without nuclear atypia (C2) and with nuclear atypia (C3) while figure 2 shows cytomorphological features of malignant breast lesions, both suspicious (C4) and confirmed (C5). These features are quite subjective and overlapping in nature. Sometimes it becomes difficult to differentiate between C3 and C4 categories while C2 and C5 categories are easier to diagnose and correlate better with their subsequent histopathological diagnosis. Lesions belonging to C3 and C4 categories are better known as Grey Zone Lesions, as they are difficult to diagnose because of inter-observer variation.
Discussion
In our present study, we included women of all age groups who presented with breast lumps or masses but having no any previous diagnosis. Benign lesions were commonly found among women belonging to age groups of 21-30 years and 31-40 years. Suspicious or Confirmed cases of malignancy were commonly found among age groups of 41-50 years and 51-60 years. Similar results were obtained in other studies like those done by Veena Kumari L et al.[2] Left sided breast lesions (60%) were more common than right sided ones (40%) and upper & outer quadrant was the commonest location (49.30% cases). In a similar study done by Kosthi A et al,[8] left sided breast lesions were found in 50.66% cases while right sided lesions were found in 40.87% cases. Rests of 8.47% cases were presented as bilateral lesions. Upper & outer quadrant was the commonest location (56.88% cases). Among other similar studies like those done by Waghmare RS et al,[9] by Zuk JA et al[10] and by Rocha PD et al,[11] upper & outer quadrant was the commonest topographical location for breast lumps and results were 42.54%, 42.20% & 45.20% respectively. So it is now obvious that age-wise distribution, site & topographical location of various breast lesions (both benign & malignant) remain more or less similar everywhere.
In this study, majority of the cases belong to C2 or benign category (53.78%) followed by those belonging to C5 or malignant category (21.37%). Study done by Veena Kumari L et al[2] shows 75.28% cases & 11.20% cases belonging to C2 and C5 categories respectively. In a similar study done by Madubogwu CI et al,[4] 41.8% of cases belong to C2 category and 34.6% cases belong to C5 category respectively. Studies done by Kosthi A et al[8] and Waghmare RS et al[9] also show similar outcomes. Atypical (C3) and suspicious (C4) categories are rare everywhere. In other words, we can say that most of the cases of breast masses are further classified into two groups only, either benign (C2) or malignant (C5). The commonest category is C2 and next common category is C5.
Statistical analysis of our present study was compared with that of other similar studies and the comparative evaluation is mentioned below in table no. 4.
Table 4: Comparative evaluation of statistical analysis of various studies
|
S.no. |
Name of the study |
Year of the study |
Sensitivity (%) |
Specificity (%) |
Positive predictive value (%) |
Negative predictive value (%) |
Overall diagnostic accuracy (%) |
|
1 |
Our present study |
2019 |
90.90 |
98.68 |
96.77 |
96.15 |
96.33 |
|
2 |
Veena Kumari L et al[2] |
2017 |
99.23 |
90.17 |
92.19 |
99.01 |
----- |
|
3 |
Madubogwu CI et al [4] |
2017 |
90.00 |
95.50 |
94.70 |
91.30 |
92.90 |
|
4 |
Kosthi A et al [8] |
2017 |
98.13 |
100.00 |
100.00 |
98.98 |
99.34 |
|
5 |
Waghmare RS et al [9] |
2016 |
88.24 |
100.00 |
100.00 |
93.26 |
95.52 |
|
6 |
Bukhari MH et al [12] |
2011 |
100.00 |
98.00 |
97.00 |
100.00 |
98.00 |
|
7 |
Choi et al [13] |
2004 |
77.70 |
99.20 |
98.40 |
88.00 |
91.10 |
|
8 |
Rocha PD et al [11] |
1997 |
93.80 |
98.21 |
92.70 |
----- |
97.40 |
|
9 |
Kapila & Verma [13] |
1989 |
97.60 |
99.40 |
99.50 |
97.20 |
98.40 |
|
10 |
Zuk JA et al [10] |
1989 |
70.60 |
87.50 |
95.20 |
----- |
----- |
All these figures mentioned above in table no. 4 suggest one fact that Fine Needle Aspiration Cytology (FNAC) is a sensitive, specific and accurate procedure for classification and pre-operative evaluation of various breast lumps or masses. FNAC itself is quite effective in initial diagnosis of various breast diseases in terms of either benign or malignant, but final diagnosis is always given after post-operative histopathological evaluation of various types of specimens like lumpectomies or mastectomies. FNAC alone has a limited role in further subclassification of various breast diseases because of certain limitations like inadequacy of aspirated material, various artifacts like air drying of smears, absence of a definite architectural pattern as seen during histopathological examination, overlapping microscopic features etc.
In our study, we have not included those cases that underwent FNAC but did not undergo subsequent histopathological diagnosis. Default rate of our present study is 32.56% (70 cases out of 215). Default rates of various other studies like those done by Madubogwu CI et al [4] and by Bukhari MH et al,[12] are 37.22% and 20.47% respectively. Patients defaulted for various reasons form a major limitation for this present study & for other similar studies.
Conclusion
Fine Needle Aspiration Cytology (FNAC) is a simple, cheap, OPD based, reliable & acceptable method for pre-operative evaluation of various breast lesions. Classification or categorization plays an important role in this evaluation and for this purpose; the National Health Services Breast Screening Programme (NHSBSP) of Britain has developed five different categories. FNAC reports put different types of breast lesions into different categories from inadequate (C1) to malignant (C5). These cytological categories show a statistically significant correlation with final diagnoses given in subsequent histopathology reports.
Conflicts of Interest: None.
References
- ^ Lod Khoda, Buru Kapa, Khuraijam Gojen Singh, Thokchom Gojendra, Laishram Ramesh Singh, Kongbrailatpam Lekhachandra Sharma. Evaluation of modified triple test (clinical breast examination, ultrasonography, and fine-needle aspiration cytology) in the diagnosis of palpable breast lumps. JMed Society 2015Jan-Apr;29(1):26-30.
- a, b, c, d, e, f, g, h Veena Kumari L, Vani R, Jijiya Bai P, K.R.K Prasad, Vijaya K. Evaluation of Breast lumps by Fine needle aspiration cytology in correlation with Histopathology. J Cont Med A Dent 2017Jan-Apr;5(1):63-67.
- ^ Norman S Williams, P Ronan O’Connell, Andrew W McCaskie. Bailey and Love’s short practice of surgery. 27th ed. Ch. 53. CRC Press, Taylor & Francis Group, 6000 Broken Sound Parkway NW, Suite 300 Boca Raton, FL 33487-2742; 2018.
- a, b, c, d Madubogwu CI, Ukah CO, Anyanwu SNC, Chianakwana GU, Onyiaorah IV, Anyiam DCD. Sub-classification of Breast Masses by Fine Needle Aspiration Cytology. Eur J Breast Health 2017;13:194-199.
- ^ Guidelines for non-operative diagnostic procedures and reporting in breast cancer screening. Non-operative diagnostic sub-group of the National Co-ordinating Group for Breast Screening Pathology. NHSBSP Publication No 50. June, 2001.18-22
- ^ Reddaiah VP, Mahajan BK. Methods in Biostatistics for medical students & research workers. 6th ed. Ch. 11. New Delhi: Jaypee brothers’ medical publishers (P) ltd.;1997.
- ^ Anthony J Viera, Joanne M Garrett. Understanding interobserver agreement: The kappa statistic. Fam Med 2005; 37(5):360-363.
- a, b, c Ashish Kosthi, Maneesh Sulya, Reeni Malik. Role of Fine-Needle Aspiration Cytology in Evaluation of Breast Lumps. Ann Appl BioSci 2017;4(3):A-143-149.
- a, b, c Ramesh S. Waghmare, Shubhangi D. Sakore, S. B. Rathod. Fine needle aspiration cytology of breast lesions and correlation with histopathology. Int J Res Med Sci 2016 Oct; 4(10): 4416-4421.
- a, b Zuk JA, Maudsley G, Zakhour H D. Rapid reporting on fine needle aspiration of breast lumps in outpatients. J Clin Pathol 1989;42:906-911.
- a, b Rocha PD, Nadkarni NS, Menezes S. Fine needle aspiration biopsy of breast lesion and histopathologic correlations, an analysis of 837 cases in four years. Acta cytol 1997;41:1131-1137.
- a, b Bukhari MH, Arshad M, Jamal S, Niazi S, Bashir S, Bakhshi IM, et al. Use of fine- needle aspiration in the evaluation of breast lumps. Pathol Res Int 2011; article ID 689521:1-10.
- a, b Kusum Verma & Kusum Kapila. The role of fine needle aspiration cytology of breast lumps in the management of patients. Indian J Med Res 1989; 90: 135-139