IP Archives of Cytology and Histopathology Research
Official Publication of Khyati Education and Research Foundation
Official Publication of Khyati Education and Research Foundation

Print ISSN: 2581-5725
Online ISSN: 2456-9267
CODEN : IACHCL
IP Archives of Cytology and Histopathology Research (ACHR) open access, peer-reviewed quarterly journal publishing since 2016 and is published under the Khyati Education and Research Foundation (KERF), is registered as a non-profit society (under the society registration act, 1860), Government of India with the vision of various accredited vocational courses in healthcare, education, paramedical, yoga, publication, teaching and research activity, with the aim of faster and better dissemination of knowledge, we will be publishing the article more...Null
Author Details :
Volume : 4, Issue : 1, Year : 2019
Article Page : 87-94
https://doi.org/10.18231/2456-9267.2019.0015

Abstract
Introduction: The role of FNA cytology is widely accepted as a reliable technique in the evaluation breast lumps.
Objectives: To study the cytology of lesions of the breast and its histopathological correlation where ever necessary and to have clinico-pathological correlation with respect to age and clinical features.
Materials and Methods: Two year prospective study, includes 110 Patients presenting with breast lumps.
Results: Maximum of 41 cases (38%) were in the age group 31-40 years. Left breast was more commonly involved with 60 cases (56%). The most common presenting symptom was a Palpable mass seen in all 108 patients. The aspirate was adequate in 108 cases (98.1%). The non neoplastic lesions accounted to 31 cases (28%). The benign conditions comprised of 59 cases (77%) and the malignant conditions comprised of 18 cases that included duct carcinoma, lobular carcinoma, Medullary carcinoma and 2 Suspicious. The 2 Suspicious cases were confirmed as malignant on histopathology. Maximum number of cases in the Non neoplastic category was seen in 21-30 years age group and the minimum was seen in the 11-20.The maximum number of cases in the Neoplastic category was seen in the 31-40 year age group with 27 cases and the minimum in the 51-60 and 61-70 year age group with three cases each.
Conclusion: FNAC on breast lumps offers many advantages to clinicians and pathologists as it is an easy and reliable method of establishing the diagnosis of various breast lesions from inflammatory to non neoplastic to malignant conditions.
Keywords: FNAC, Breast-Non noplastic and Neoplastic lesions.
With growing awareness in the general population about breast pathologies, a lady with breast lump is one of the most common presentations in the outpatient department[1].
Various benign and neoplastic lesion of the breast may present for needle aspiration. The spectrum of lesions of the female breast are classified as Inflammatory lesions, lesions caused by trauma, Benign Proliferative disorders, Benign tumors, Malignant tumors and Metastatic tumors.[2]
The fine needle aspiration cytology has become the investigation of choice for the diagnosis of the breast malignancy. FNAC is widely accepted as a reliable technique as the procedure is simple, safe, cost effective, minimally invasive, rapid, and causes minimal morbidity. Hence, an attempt is made to diagnose the spectrum of Non neoplastic and neoplastic lesions of the breast by fine needle aspiration cytology, in our institute.
To study the cytology of lesions of the breast and its histopathological correlation where ever necessary and to have clinico-pathological correlation with respect to age and clinical features.
Source of Data: All female patients presenting with Non neoplastic and neoplastic breast lesions attending Hospital and other peripheral referral centers are the subjects of the study.
Methods of collection of data: All the patients referred to the department of pathology, Navodaya Medical College Hospital and Research center and from peripheral referral centres, for FNAC of breast lesions were enrolled for the study. The patients were clinically evaluated, and the details were obtained. FNAC was done and the standard method for the procedure was adopted. All the slides were reviewed and their diagnosis was made according to their respective criteria.
Study Period: A two year cross sectional study with desired sample size of 100 cases
Inclusion Criteria: All female patients presenting with lesions of the breast aged between 15 and 70 years are included in the study.
Exclusion criteria: Patients’ refusal / non willingness for the procedure, male patients, aspirates with paucicellularity, hemorrhagic acellular smears, Patients presenting with lesions of the skin of the breast, lesions of the chest wall, lymph nodes in the axillary tail of the breast, are excluded from the study.
Breast slides were systemically evaluated for the following features
Results
This study comprised of a total number of 110 cases, which included both Non neoplastic and Neoplastic lesions of the breast. 2 cases were considered as inconclusive and excluded from the study. The remaining 108 cases were included in the study, where Non neoplastic lesions of the breast accounted to 31 cases (28%) and Neoplastic lesions to 77 cases (71.3%).
Age of the patients of the cases in the study ranged from 15 to 70 years. The maximum number of 41 cases (38%) was seen in the age group of 31-40 years, and the minimum number of 3 cases (2.8%) was seen in the age group of 51-60 years.
Presenting Symptoms: Clinical evaluation of all the cases were done in this study which showed most common symptoms like palpable mass in all 108 cases (100%), followed by mastalgia - 60 cases (56%) while the least common symptom was nipple discharge - 5 cases (4.7%),
Incidence of non neoplastic lesions: Non neoplastic lesions of the breast in the present study accounted to 31cases (28%) of the total 108 cases. Of the 31 cases, according to the decreased order of frequency, the lesions were, Acute mastitis - 13 cases (42%), Fibrocystic disease - 9 cases (29%), Simple cyst – 4 cases (13%), Galactocele –1 case (3.2%), Chronic mastitis –1 case (3.2%), Granulomatous mastitis – 1case (3.2%), Duct ectasia -1 case (3.2%) and Fat necrosis – 1 case (3.2%).
Table 1: Incidence of non neoplastic breast lesions
|
S. no. |
Non neoplastic lesions |
Number of cases |
Percentage |
|
1. |
Acute mastitis |
13 |
42.00% |
|
2. |
Fibrocystic disease |
09 |
29.0 % |
|
3. |
Simple cyst |
04 |
13% |
|
4. |
Galactocele |
01 |
3.2% |
|
5. |
Chronic mastitis |
01 |
3.2 % |
|
6. |
Granulomatous mastitis |
01 |
3.2% |
|
7. |
Duct ectasia |
01 |
3.2% |
|
8. |
Fat necrosis |
01 |
3.2% |
|
|
Total |
31 |
100.00 |
Incidence of meoplastic lesions
Of the total 108 cases in this study, Neoplastic lesions comprised of 77 cases (71.3%) among which, Benign lesions were 59 cases (77%) and the Malignant were 18 cases (23.4%).
Benign Lesions: The Benign lesions comprised of 59 cases (77%) out of 77 Neoplastic lesions and the incidence
according to the decreased order of frequency, were Fibroadenoma with 45 cases (76.3%), Benign duct hyperplasia – 11 cases (18.6%), Benign Phyllodes tumor - 1 case (1.7%), Lipoma - 1 case (1.7%) and Atypical duct hyperplasia - 1 case (1.7%).
Table 2: Incidence of benign lesions
|
S. no. |
Benign Lesions |
Number of cases |
Percentage |
|
1. |
Fibroadenoma |
45 |
76.3% |
|
2. |
Benign duct hyperplasia |
11 |
18.6% |
|
3. |
Benign phyllodes tumor |
1 |
1.7% |
|
4. |
Lipoma |
1 |
1.7% |
|
5. |
Atypical duct hyperplasia |
1 |
1.7% |
|
|
Total |
59 |
100.0% |
Malignant Lesions
The Malignant lesions comprised of 18 (23.4%) out of 77 Neoplastic lesions. Of the 18 cases, 16 were diagnosed as malignant on cytology and 2 were considered in the Suspicious category. Of the 16 cases diagnosed as malignant on cytology, 14 (77.7%) were Invasive duct carcinoma of
the NOS type, 1 case (5.6%) was of Invasive lobular carcinoma and 1 case (5.6%) of Medullary carcinoma.
The 2 remaining cases (11.1%) which were considered as Suspicious for malignancy, were finally confirmed as
Invasive duct carcinoma – NOS in both the cases, after subjecting them to histopathological examination.
Table 3: Age distribution of non neoplastic breast lesions
|
Non neoplastic lesions |
11-20 |
21-30 |
31-40 |
41-50 |
51-60 |
61-70 |
Total |
|
Acute mastitis |
1(7.7%) |
8(61.5%) |
4(31%) |
|
|
|
13 |
|
Galactocele |
|
1(100%) |
|
|
|
|
1 |
|
Chronic mastitis |
|
|
|
|
|
1(100%) |
1 |
|
Granulomatous mastitis |
|
1(100%) |
|
|
|
|
1 |
|
Duct ectasia |
|
|
1(100%) |
|
|
|
1 |
|
Fat necrosis |
|
1(100%) |
|
|
|
|
1 |
|
Fibrocystic disease |
|
2(22.2%) |
7(77.7%) |
|
|
|
9 |
|
Simple cyst |
|
2(50%) |
2(50%) |
|
|
|
4 |
|
Total |
1 |
15 |
14 |
|
|
1 |
31 |
?2 = 0.671, df=1, p=0.413
Table 4: Age distribution of neoplastic breast lesions
|
Neoplastic lesions |
11-20 years |
21-30 years |
31-40 Years |
41-50 Years |
51-60 Years |
61-70 Years |
Total |
|
Benign |
|
|
|
|
|
|
|
|
Fibroadenoma |
12(26.6%) |
16(35.5%) |
14(31.1%) |
2(4.4%) |
1(2.2%) |
|
45 |
|
Benign Phyllodes |
|
|
|
1 (100) |
|
|
1 |
|
Lipoma |
|
1 (100) |
|
|
|
|
1 |
|
Benign duct hyperplasia |
|
1(9.1%) |
8(72.7%) |
2(18.2%) |
|
|
11 |
|
Atypical duct hyperplasia |
|
|
|
|
1 (100) |
|
1 |
|
Malignant |
|
|
|
|
|
|
|
|
Invasive duct carcinoma |
|
1(7.14%) |
4(28.6%) |
6(43%) |
1(7.14%) |
2(14.3%) |
14 |
|
Invasive lobular carcinoma |
|
|
1(100%) |
|
|
|
1 |
|
Medullary carcinoma |
|
|
|
|
|
1(100%) |
1 |
|
Suspicious |
|
|
|
2(100%) |
|
|
2 |
|
Total |
12 |
19 |
27 |
13 |
3 |
3 |
77 |
?[2] = 13.55,df=1, p=0.0002
Out of a total number of 108 cases, 38 cases were subjected for histopathological examination that included 2 Non neoplastic lesions and 36 Neoplastic lesions.
In the Nonneoplastic category, out of 2 cases available for histopathological correlation, 1 correlated and was a case of Granulomatous mastitis. The other case which did not correlate was a case of Invasive Duct carcinoma NOS (Mixed type) which was initially diagnosed on cytology as Fibrocystic disease.
In the Neoplastic category, 24 cases of Benign lesions and 12 cases of malignant lesions had histopathology slides available for correlation.
Of the 24 benign lesions, 23 cases showed good correlation and 1 did not correlate. Out of 23 cases that showed correlation, 20 cases were of Fibroadenoma and the remaining 3 cases were of Phyllodes tumor, Lipoma and Atypical duct hyperplasia, comprising of one case each. One case that did not show correlation was initially diagnosed as Benign duct hyperplasia on cytology and was confirmed as Atypical duct papilloma on histopathology.
 |
Click here to view |
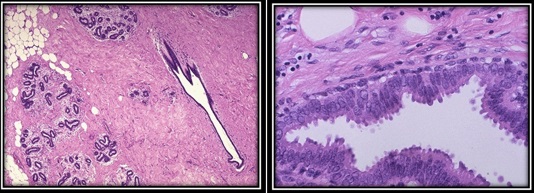
Fig. 1 & 2.Histology of normal female breast with ducts/ lobules in a fibrous stroma with adipose tissue.(Left side, H&E,10x) and Normal breast acinus showing epithelial cells lining the lumen with apocrine secretion(Right Side
 |
Click here to view |
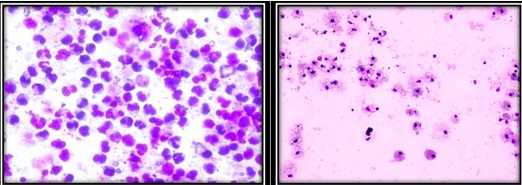
Fig. 3: & 4: Acute mastitis: Sheets of neutrophils with duct cells (MGG,40x) & Simple cyst: Foamy macrophages with scattered duct cells (MGG, 10x)
 |
Click here to view |
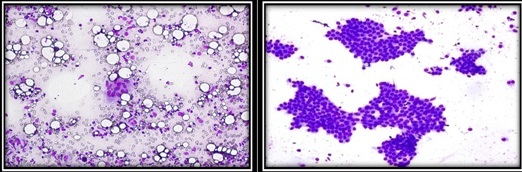
Fig. 5: & 6: Granulomatous mastitis: A multinucleated giant cell along with scattered breast ductal cells and fat cells. (MGG,10x) Fibroadenoma: Staghorn pattern of duct cells with bare nuclei in the background.(MGG,10x).
 |
Click here to view |
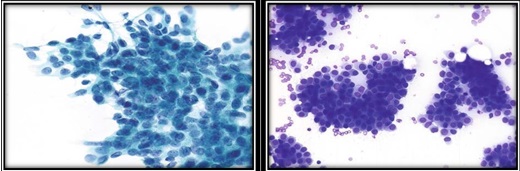
Fig. 7: & 8: Atypical ductal hyperplasia: Cellular fragment displaying pleomorphism with enlarged crowded nuclei and focal three- dimensional architecture. (Pap, 40x) Ductal carcinoma: Tumor cells in irregular fragments, loosely arranged and displaying uniform “plasmacytoid” appearance (MGG,10x)
Discussion
Fine needle aspiration of the breast is one of the most valuable diagnostic tools in the assessment of benign and malignant lesions.[3]
Patients with breast lesions underwent FNAC and with adequate aspirate accounted to 108 cases in the present study of 2 years, between August 2009 and August 2011.
The age incidence of the patients with breast lesions varied from 15-70 years. The maximum incidence of 41 cases (38%) was seen in the age group of 31-40 years and the minimum -3 cases (2.8%) were seen in the age group of
51-60 years. Studies conducted by Rocha P D et al[4] also reported similar incidences (40.7%) with respect to 31-40 years age group, whereas Talpur K.A.H et al[5]and Kumar R[6]
on the contrary, documented maximum incidences (28% and 36%) in the age group of 11-20 years and 21-30 years, respectively.
The minimum incidence of cases in the present study correlated with the study of K.A.H. Talpur et al[5] and Kumar R[6](3.33% and 2.0%) in 61-70 years age group, on the contrary, Rocha P D et al[4] recorded a slightly higher incidence (9.1%) in the age group of 51-60 years.
Table 5: comparison of incidence of presenting symptoms of the present study with various studies
|
Breast symptoms |
Talpur KAH [5] |
Kumar M et al[7] |
Bell D A[8] |
Present study |
|
Palpable mass |
100% |
84.1% |
88.9% |
100.0% |
|
Mastalgia |
53.33% |
64.7% |
5.12% |
56.0% |
|
Nipple discharge |
3.33% |
5.5% |
- |
4.70% |
Comparison of incidence of non neoplastic lesions in present study with various studies
In the present study, the Non neoplastic breast lesions accounted to 31 cases (28%) of the total 108 cases and the incidence according to the decreased order of frequency were Acute mastitis (42%), Fibrocystic disease (29%), Simple cyst (13%), Galactocele (3.2%), Chronic mastitis (3.2%), Granulomatous mastitis (3.2%), Duct ectasia (3.2%) and Fat necrosis (3.2%).
Acute mastitis: The incidence of Acute mastitis (42%) is one of the predominant Non neoplastic lesions in this study which nearly correlated with the observation of Malik M[9](36.1%) while lower incidences of the lesion were reported by Tiwari M et al (21.4%)[10], and Pradhan M (11.5%).[11]
Galactocele: Galactocele in our study accounted to 3.2% and was comparable to the study of Malik M (3.81%),[9] but was significantly higher in the studies of Amr SS[12] and Tiwari M[10] and Singh A et al [13], who reported incidences of 5.7%, 18% and 17.5% respectively. In contrast, Singh K[14] and Pradhan M[11] reported lower incidences of 1.8% and 1.1% respectively, when compared to the present study.
Chronic mastitis: In the present study, Chronic Mastitis accounted to 3.2% and correlated with the study of Amr SS (2.8%)[12] whereas Qasim M et al[15]and Malik M. et al[9] reported significantly higher incidences accounting to 44.4% and 8.47%, respectively.
Granulomatous mastitis: Granulomatous mastitis accounted to 3.2% in the present study, which corroborated with the study of Malik M. et al (2.96%),[9]but studies conducted by Amr SS (4.1%),[12] Singh K (4.7%)[14]and Qasim M et al (11.1%)[15]reported higher incidences while Pradhan M (0.6%)[11] reported a lower incidence when compared to the present study.
Duct ectasia: The incidence of Duct ectasia in our study was 3.2% and was significantly lower when compared with the studies conducted by Amr SS[12], Tiwari M [10]and Malik M. et al[9]who reported significantly higher incidences of 11.7%, 17.9% and 19.49% respectively, while Pradhan M[11]reported a lower incidence of 1% compared to this study.
Fat necrosis: In the present study, the incidence of Fat necrosis was 3.2% which was lower when compared with the studies of Singh K[14]and Qasim M et al[15] who reported significantly higher incidences of 5.7% and 22.2% respectively.
Fibrocystic disease: Fibrocystic disease in our study accounted to 29% of cases, which correlated with the findings of Qasim M et al (22.2%),[15] Malik M. et al (27.1%)[9]and Singh A et al (30%),[13] whereas Amr SS[12]reported a significantly higher incidence of 50.5% in their study while lower incidence of this lesion were documented by Tiwari M (17.9%)[10] and Pradhan M et al (7%)[11] when compared to the present study.
Simple cyst: The incidence of Simple cyst (13%) in the present study was higher compared to the findings of Pradhan M et al (2.2%).[11]
Comparison of incidence of neoplastic lesions of the present study with various studies
Of the total 108 cases in this study, Neoplastic lesions comprised of 77 cases (71.3%) among which, Benign lesions were 59 cases (77%) and the Malignant were 18 cases (23.4%).
Benign lesions: In the present study, the incidence of various benign lesions in the decreasing order of frequency were Fibroadenoma (76.3%), Benign duct hyperplasia (18.6%), Benign Phyllodes tumor (1.7%), Lipoma (1.7%) and Atypical duct hyperplasia (1.7%).
Fibroadenoma: Fibroadenoma was the predominant benign lesion in this study accounting to 76.3% which was consistent with the observation of Amr SS[12](74%) whereas Tiwari M[10](97.2%) and Pradhan M. et al[11] (91.3%), reported higher incidences compared to the present study. Malik M [9] on the other hand reported comparatively lower incidence of 58.51%.
Benign Phyllodes tumor: The incidence of Benign Phyllodes tumor in the present study (1.7%) corroborated with the study of Pradhan M. et al[11]who reported a similar incidence (2%), while lower incidences were reported by Amr SS[12] and Malik M[9] (0.7% and 0.6% respectively) when compared to the present study.
Lipoma: A case of Lipoma with an incidence of 1.7% was observed in the present study, which was lower compared to the studies of Amr SS[12] and Pradhan M. et al[11]who reported slightly higher incidences of 3.4% and 3.5% respectively.
Benign duct hyperplasia: The incidence of Benign duct hyperplasia of 18.6% in the present study was significantly higher when compared to the findings of Dahri F J et al,[16] who reported a much lower incidence of 3.2%.
Atypical duct hyperplasia: The incidence of Atypical duct hyperplasia in the present study (1.7%) was comparable to the studies of Tiwari M[10]and Pradhan M. et al,[11]who showed similar incidences of 2.7% and 3% respectively.
Comparison of incidence of malignant lesions in the present study with various studies
The Malignant lesions comprised of 18 (23.37%) out of 77 Neoplastic lesions. Of the 18 cases, 16 were diagnosed as malignant on cytology and 2 were considered in the Suspicious category. Of the 16 cases diagnosed as malignant on cytology, 14 cases (77.7%) were Invasive duct carcinoma of the NOS type, one case (5.6%) of Invasive lobular carcinoma and a case (5.6%) of Medullary carcinoma.
The two remaining cases (11.1%) which were considered as Suspicious for malignancy, were finally confirmed as Invasive duct carcinoma – NOS (Mixed subtype) in both the cases, after subjecting them to histopathological examination.
Invasive duct carcinoma: The incidence of Invasive ductal carcinoma in the present study was 77.7% which corroborated with the study of Rocha PD et al[4](79.2%) while Singh K et al (85%)[14] reported a slightly higher incidence. But contradictory to our study, Malik M et al[9] reported a significantly lower incidence (30.5%) of this lesion.
Invasive lobular carcinoma: The incidence of Invasive Lobular carcinoma in the present study was 5.6% whereas the study of Malik M[9](8.1%) reported a slightly higher incidence, while Amr SS[12]reported a lower incidence of 2.2% when compared to the present study.
Medullary carcinoma: A case of Medullary carcinoma with an incidence of 5.6% was reported in the present study which corroborated with that of Amr SS[12](5.03%), while Malik M[9]reported a slightly higher incidence of 12% when compared with our study.
Suspicious: The cases categorized as Suspicious which has an incidence of 11.1% in the present study was consistent with the findings of Singh K et al (12.5%)[14], but the study by Rocha PD et al (21%)[4] reported a significantly higher incidence while Malik M et al[9] reported a much lower incidence (0.4%) when compared to the present study.
Comparison of age distribution of non neoplastic breast lesions in the present study with various studies.
Acute mastitis: In the present study, highest number of cases of Acute mastitis was seen in the age group of 21-30 years which was comparable to the studies conducted by Amr S S et al,[12] Khanzada T W et al[17] and Dahri F J et al,[16] who also reported maximum number of cases in the same age group.
Galactocele: The age group for maximum number of cases of Galactocele in the present study which was 21-30 years correlated with the study of Dahri F J et al[16]who also reported the highest number of cases in the same age group.
Chronic mastitis: In the present study one case of Chronic mastitis was reported at a much higher age group of 61-70 year which varied with the study conducted by Amr SS[12]who reported a lower age of occurrence of the lesion at 28 years.
Granulomatous mastitis: A case of Granulomatous mastitis seen in the present study was reported in the age group of 21-30 years which corroborated with the studies of Khanzada T W et al[17]and Dahri F J et al[16]who also reported the maximum number of cases of the lesion in the above said age group, whereas Amr SS[12]reported maximum number of cases at the age of 41 years, compared to the present study.
Duct ectasia: Highest number of cases of Duct ectasia in the present study was reported in the age group of 31-40 years which corroborated with the studies conducted by Khanzada T W et al[17] and Dahri F J et al[16] who also reported maximum number of cases in the same age group. This was in contrast to Amr SS[12]who reported maximum cases at a higher age of 51 years.
Fat necrosis: A case of Fat necrosis was reported in the present study in the 21-30 years age group in contrast to the study conducted by Khanzada T W et al[17]who reported maximum number of cases at a higher age group of 31-40 years.
Fibrocystic disease: Highest number of cases of Fibrocystic disease in the present study were described in the age group of 31-40 years which was similar to the studies of Khanzada T W et al[17]and Dahri F J et al[16] who also reported increased number of cases of the lesion in the said age group.
Simple cysts: Maximum number of cases of Simple cysts were reported in the 31-40 years age group in the present study which were comparable to that of the study of Hindle W et al[18]who also reported maximum cases at the age of 37 years.
Comparison of age distribution of neoplastic lesions in the present study with various studies
Benign
Fibroadenoma: The maximum number of cases of Fibroadenoma in the present study was seen in the 21-30 year age group which was consistent with the studies conducted by Amr SS et al[12], Khanzada T W et al[17] and Dahri F J et al[16] who also observed highest number of cases in the same age group.
Benign Phyllodes tumor: A case of Benign Phyllodes tumor was described in the 41-50 years age group which correlated with that of Malik M[9]who reported the lesion at an age of 39 years whereas Rao C R[19]reported the lesion at a slightly lower age of 35 years.
Lipoma: A case of Lipoma was observed in the age group of 21-30 years in the present study which was in contrast to the study conducted by Amr SS et al[12] who reported the lesion at a much higher age of 44 years.
Benign duct hyperplasia: The maximum number of cases of Benign duct hyperplasia in this study were reported in the age group of 31-40 years which corroborated with the findings of Dahri F J et al[16]who also reported the highest number of cases of the same lesion in the said age group.
Atypical ductal hyperplasia: A case of Atypical ductal hyperplasia was described in the 51-60 year age group in the present study which corroborated with the study conducted by Sneige N et al[20]who reported the lesion at an age of 55 years.
Table 6: Comparison of age distribution of benign lesions in the present study with various studies
|
Benign Lesions |
Rao CR et al19 1992 |
Sneige N et al20 1994 |
Amr SS et al12 1995 |
Khanzada T W et al17 2009 |
Dahri F J et al16 2010 |
Malik M et al9 2010 |
Present study |
|
Fibroadenoma |
- |
- |
21-30 |
21-30 |
21-30 |
- |
21-30 |
|
Benign Phyllodes tumor |
35
|
- |
- |
- |
- |
39 |
41-50 |
|
Lipoma |
- |
- |
44 |
- |
- |
- |
21-30 |
|
BDH |
- |
- |
- |
- |
31-40 |
- |
31-40 |
|
ADH |
- |
55 |
- |
- |
- |
- |
51-60 |
Comparison of age distribution of malignant lesions in the present study with various studies
Invasive Duct carcinoma: The maximum number of cases of Invasive duct carcinoma in the present study was seen in the age group of 41-50 years which was similar to the Studies conducted by both Amr SS et al[12]and Malik M[9] who also reported the highest number of cases of the same lesion in the same age group. Another similar study conducted by kumar R[6]also found the highest number at an age of 54 years.
Invasive lobular carcinoma: A case of Invasive lobular carcinoma described in the present study was seen in the age group of 31-40 while both Malik M[9]and Amr SS et al[12]
reported maximum cases of the same at a higher age group of 41-50 years.
Medullary carcinoma: One case of Medullary carcinoma described in the present study was reported in the age group of 61-70 years, while studies conducted by both Malik M[9]and Amr SS[12]reported the lesions at a lower age group of 41-50years.
Suspicious of Malignancy: All the cases of Suspicious category in the present study were described in the age group of 41-50 years which were comparable to the study conducted by Rocha PDS[4]who also showed the highest number of cases in the same age group.
Table 7: comparison of age distribution of malignant lesions in the present study with various studies
|
Malignant Lesions |
Amr SS et al[12](1995) |
Rocha PDS[4](1997) |
kumar R[6] (2010) |
Malik M[6] (2010) |
Present study |
|
Invasive duct carcinoma |
41-50 |
- |
54 |
41-50 |
41-50 |
|
Invasive lobular carcinoma |
41-50 |
- |
- |
41-50 |
31-40 |
|
Medullary carcinoma |
41-50 |
- |
- |
41-50 |
61-70 |
|
Suspicious |
- |
41-50 |
- |
- |
41-50 |
Correlation of FNAC and histopathology
Out of a total number of 108 cases, 38 cases were subjected for histopathological examination which included 2 Non neoplastic and 36 Neoplastic breast lesions. Of the total 38 cases, 34 cases showed good correlation.
In the Non neoplastic category, out of 2 cases available for histopathological correlation, one correlated and was a case of Granulomatous mastitis. The other case that did not correlate was a case of Invasive duct carcinoma- NOS (Mixed type) which was initially diagnosed as fibrocystic disease on cytology.
In the Neoplastic category, 24 cases of benign lesions and 12 cases of malignant lesions were available for histopathological correlation.
Of the 24 cases of benign lesions available for histopathological correlation, 23 cases showed good correlation and one case did not correlate. Of the 23 cases which correlated, 20 cases were of Fibroadenoma and the remaining were benign phyllodes tumor, lipoma and atypical duct hyperplasia, comprising of one case each. The case that did not show correlation was a case of Atypical duct papilloma, which was initially diagnosed as Benign duct hyperplasia on cytology.
Conclusions
The present study was undertaken to know the FNAC of breast lesions and compare the results of FNAC with that of histopathology and also to study and assess clinicopathologic features of breast lesions.
Breast cytology, particularly fine needle aspiration Cytology (FNAC), has been an integral part in the management of women with breast lesions and FNAC is a simple, cost effective and less traumatic method for diagnosis of breast lump.
So we recommend that FNAC of breast lump should be used as preliminary investigation in outdoor patient department as well as a routine method for determining the nature of breast
Conflict of Interest: None.
How to cite : David H, Patil M S, Anand A S, Fine needle aspiration study of non neoplastic and neoplastic breast lesions. IP Arch Cytol Histopathol Res 2019;4(1):87-94
This is an Open Access (OA) journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.