IP Archives of Cytology and Histopathology Research
Official Publication of Khyati Education and Research Foundation
Official Publication of Khyati Education and Research Foundation

Print ISSN: 2581-5725
Online ISSN: 2456-9267
CODEN : IACHCL
IP Archives of Cytology and Histopathology Research (ACHR) open access, peer-reviewed quarterly journal publishing since 2016 and is published under the Khyati Education and Research Foundation (KERF), is registered as a non-profit society (under the society registration act, 1860), Government of India with the vision of various accredited vocational courses in healthcare, education, paramedical, yoga, publication, teaching and research activity, with the aim of faster and better dissemination of knowledge, we will be publishing the article more...Null
Author Details :
Volume : 4, Issue : 1, Year : 2019
Article Page : 95-98
https://doi.org/10.18231/2456-9267.2019.0016

Abstract
Simple renal cysts are the most common renal masses but the major concern is to differentiate a simple renal cyst from a complex cyst which may have foci of malignancy. However, this association is seen in 1% cases only. Most of the renal cysts are benign, asymptomatic and are usually treated conservatively. However, various cystic diseases are associated with renal cell carcinoma. Renal cysts with thickened, irregular septa and enhancement on contrast injection raise a suspicion of malignancy. We present a case of a 41 year old male who presented with renal cell carcinoma of left kidney with multiple simple renal cysts.
Keywords: Multifocal RCC, Nephrectomy, Renal cyst, Renal cell carcinoma.
Risk factors for Renal Cell Carcinoma (RCC) includes cystic diseases like Adult Polycystic Kidney Disease (APCKD), acquired cystic diseases, Von-Hippel Lindau (VHL) disease and tuberous sclerosis complex (TSC).[1],[2]Risk of RCC in ADPKD is not known exactly. On the other hand, risk of RCC in VHL patients is substantial and mortality rate is also high despite close follow-up. In tuberous sclerosis complex patient’s risk of development of RCC is far less as compared to the risk in VHL patients.[3]In cysts with a nodule, cystic tumour necrosis and intrinsically cystic neoplasms, the adjacent kidney tissue is mostly non-cystic. However, if multiple renal cysts are present, a cystic renal disease with a neoplastic diathesis should be considered and investigated. We present a case of 41 year old male patient who presented with RCC of left kidney in association with multiple simple renal cysts.
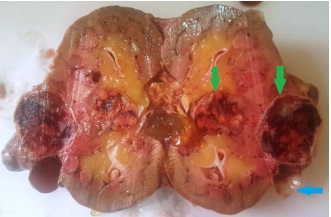
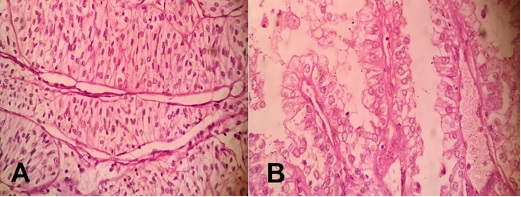
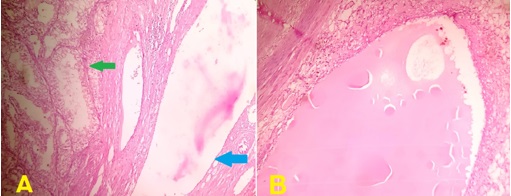
A 41 year old male presented with lower back pain for 4 months. Ultrasound showed multiple solid and cystic lesions in left kidney and diagnosis was given as likely to be RCC. Left radical nephrectomy was done and renal specimen was received in histopathology measuring 8.5x7x6cm. External surface showed numerous cysts ranging in size from 1.8x1.5cm to 1x0.8cm. (Fig. 1) The cysts were thin-walled and filled with gelatinous material to clear fluid. On bisecting the kidney, two well-circumscribed growths measuring 4x3x3cm and 2.2x2x1.2cm were seen in the middle part and near the pelvis, respectively. The cut section of both the growth was variegated and showed areas of hemorrhage and necrosis. (Fig. 2) Microscopic examination from both the growth showed round to polygonal tumor cells with abundant clear cytoplasm, arranged in solid sheets and tubules. (Fig. 3A) These tumor cells were traversed by delicate branching vasculature. Focal area showed clear cells arranged in papillary fashion with fibrovascular core present in papillae. (Fig. 3B). At places tumor cells were forming tubular structure with presence of simple cyst adjacent to the tumor. (Fig. 4A) Multiple simple renal cysts lined by cuboidal epithelium and filled with proteinaceous material were identified in the adjacent renal tissue. (Fig. 4B) Thus, based on histopathological examination a diagnosis of Multifocal RCC, Clear cell type with focal papillary features with presence of multiple simple renal cyst was rendered. Furham’s nuclear grade of the neoplasm was 2. Pathological TNM staging was T1NX. Ureter, renal vein and perinephric fat were found to be free of tumour.
 |
Click here to view |
Fig. 1: Gross- Left radical nephrectomy specimen showing grey white nodular tumor mass (Green arrow) along with many variably sized simple renal cyst (Blue arrow).
 |
Click here to view |
Fig. 2: Gross- On bisecting the kidney, two well-circumscribed growth was seen in the middle part and near the pelvis. The cut section of both the growth was variegated and showed areas of hemorrhage and necrosis (Green arrow). A thin walled cyst is also seen adjacent to larger growth (Blue arrow).
 |
Click here to view |
Fig. 3: A- photomicrograph showing sheets of round to polygonal tumor cells with abundant clear cytoplasm along with traversing delicate branching vasculature (H&Ex400). B- Photomicrograph showing papillary arrangement of clear tumor cells (H&Ex400).
 |
Click here to view |
Simple renal cyst is the most common pathology associated with urinary tract system. However, Renal Cell Carcinoma is seen to be associated with multiple simple renal cysts in only 1% cases.[3]Case reports of this association are very rare. In the year 1875, association
between Renal Cell Carcinoma (RCC) and simple renal cysts was first proposed by Sturm.[4]
Mostly the simple renal cysts are unilocular and benign whereas the complex cysts have thickened irregular septa & may be multiloculated. Recent advances in radiology have improved the clinical approach towards diagnosing the asymptomatic renal masses. Bosniak classification system clinically classifies the renal cystic tumors into 3 categories based on the CT findings. In category I, the incidence of malignancy is very low whereas in categories II and III, a certain risk of malignant cystic disease is included and appropriate treatment may be required.[5],[6]However, it may be difficult to determine preoperatively whether or not a cyst is malignant due to the small size of the malignant tissue inside the cyst, which cannot be detected by imaging alone.
Lin et al, reported a case which was initially diagnosed as a simple cyst and was treated by ultrasound?guided aspiration, but 3 weeks later ultrasound examination revealed a recurrent sizeable cyst which was treated by performing nephrectomy. The pathological examination confirmed the diagnosis of papillary RCC.[7] Visapaa et al, evaluated 482 patients and demonstrated an association between simple renal cysts and papillary RCC.[8] Sakai et al, reported a case of a simple renal cyst that developed into a septated renal cyst and finally transformed into a cystic clear cell RCC over a duration of 6 years.[9]This case demonstrated the natural transformation of a simple renal cyst into malignancy and emphasized that careful follow?up of renal cysts, particularly of complicated type, is mandatory. Takao et al, also reported a similar case where cystic RCC was diagnosed as a simple cyst preoperatively.[10]
Both acquired and syndromic renal cysts may be associated with Renal Cell Carcinomas such as Adult Polycystic Kidney Disease (APCKD), Von-Hippel Lindau (VHL) disease and tuberous sclerosis complex (TSC). A study conducted by Keith et al found that in association with Autosomal Dominant Polycystic Kidney Disease, Renal Cell Carcinoma develops at a younger age (47 years) as compared to sporadic Renal Cell Carcinoma (61 years). Also, it is more often bilateral (12 versus 2 to 6%) and multicentric (30 versus 5%).[11]Breysem L et al, observed that in Tuberosus Sclerosis Complex cases, renal involvement occurs in 50 to 80% cases in the form of rnalignant cysts and renal neoplasms.[12]
Shehata BM et al, observed that in Von-Hippel Lindau patients, renal involvement occurs in the form of multiple, bilateral clear cell-lined cysts in 70 to 80% cases and multiple, bilateral clear cell type Renal Cell Carcinoma in 40-60% cases.[13],[14]Association between Renal Cell Carcinoma and End Stage Kidney Disease with Autosomal Dominant Polycystic Kidney Disease was first proposed by Dunhill et al.[15] In End Stage Kidney Disease and Autosomal Dominant Polycystic Kidney Disease patients the risk of developing Renal Cell Carcinoma increases with the duration of dialysis. The neoplasms developing in End Stage Kidney Disease and Autosomal Dominant Polycystic Kidney Disease are more often multifocal, bilateral and have a papillary appearance.[16],[17]Renal Cell Carcinoma associated with End Stage Kidney Disease has now been recognized as a distinct entity by World Health Organization (WHO). Also risk of RCC in acquired renal cystic disease is five times greater than in the general population. The morphology of the cysts and associated tumor types can help to predict the acquired or genetic basis of the lesions. Thus, it is important to mention these associations in the histopathology reports.[18]
Understanding of the initiating molecular events in cyst formation & renal neoplasm in cystic diseases like Adult Polycystic Kidney Disease (APCKD), acquired cystic diseases, Von-Hippel Lindau (VHL) disease and tuberous sclerosis complex (TSC) is important as it has shown promise for developing targeted therapies for neoplasms which were previously being treated by surgical approach.
The aim of the present study was to emphasize the importance of recognizing that RCC may occur in what appears to be a simple renal cyst. Although, this association of RCC with simple renal cysts is seen in only one percent of cases, if the presence of malignancy is pathologically confirmed, an immediate partial or radical nephrectomy needs to be performed.
Conflicts of Interest: None.
How to cite : Hassan M J, Bajaj A, Khan S, Abeer I, Jetley S, Multifocal renal cell carcinoma associated with multiple simple renal cysts: A rare presentation. IP Arch Cytol Histopathol Res 2019;4(1):95-98
This is an Open Access (OA) journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.