IP Archives of Cytology and Histopathology Research
Official Publication of Khyati Education and Research Foundation
Official Publication of Khyati Education and Research Foundation

Print ISSN: 2581-5725
Online ISSN: 2456-9267
CODEN : IACHCL
IP Archives of Cytology and Histopathology Research (ACHR) open access, peer-reviewed quarterly journal publishing since 2016 and is published under the Khyati Education and Research Foundation (KERF), is registered as a non-profit society (under the society registration act, 1860), Government of India with the vision of various accredited vocational courses in healthcare, education, paramedical, yoga, publication, teaching and research activity, with the aim of faster and better dissemination of knowledge, we will be publishing the article more...Null
Author Details :
Volume : 4, Issue : 1, Year : 2019
Article Page : 99-101
https://doi.org/10.18231/2456-9267.2019.0017

Abstract
Endometriosis is defined as the presence of endometrial tissue outside the endometrium and myometrium. Endometriosis is a relatively less common disease. Perianal endometriosis is a very rare entity. The lesion is usually localised in the episiotomy scars and uncommonly associated with cyclical pain. Here a case of perianal endometriosis in a 30 year old female patient having painful perianal swelling, who had a history of episiotomy is being reported. Clinically diagnosed as perianal abscess, the lesion was treated surgically by wide margin excision. Histopathological examination revealed presence of endometriotic tissue, composing of endometrial glands surrounded by endometrial stromal cells. Presence of endometrial stromal cells is confirmed by CD10 marker during IHC. Thus the histomorphological and IHC findings were consistent with the diagnosis of perianal endometriosis.
Keywords: Endometriosis, Perineum, Pain, Abscess, CD10.
Endometriosis is defined as the presence of endometrial tissue outside the endometrium and myometrium.[1] The most common anatomical sites of endometriosis are the ovaries, the uterosacral, broad, or round ligaments, the rectovaginal septum, cul-de-sac, fallopian tubes, and other pelvic organs. Endometriosis may occur rarely at the scar sites following operations in the lower abdominal wall on the uterus, fallopian tubes and episiotomy. Very rarely endometriosis can be seen in the perianal region (0.2% of ectopic endometriosis); mostly in the episiotomy scar.[1],[2]
Endometriosis can manifest with a spectrum of symptoms ranging from chronic pelvic pain to infertility; but has been known to be asymptomatic in a small proportion of cases.[1] Clinical picture of scar endometriosis is typically a swelling or a nodule seen, a few weeks to years after surgery. Examination of the lesion reveals tenderness and occasional bleeding. Perianal endometriosis can clinically mimic an abscess as a result of the presence of tenderness. Atypical manifestation also includes absence of cyclical pain.[2] Endometriosis is identified histologically by the presence of endometrial glands, surrounded by endometrial stromal cells and hemosiderin laden macrophages. Endometrial stromal cells express CD10 marker. Hence CD10 marker can be used to detect occult or inconspicuous ectopic endometrial stromal cells.[3],[4]
Here, a case of perianal endometriosis in a thirty year old female patient is being reported.
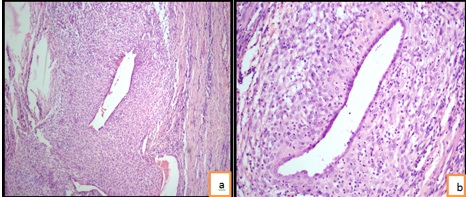
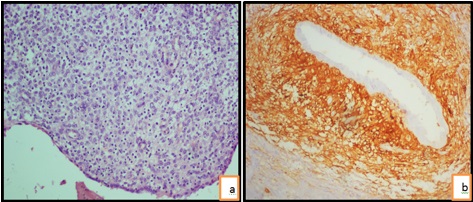
A thirty year old female came with complaints of a painful swelling in the perianal region since 4 years which had aggravated since last 3 months. The pain was dull aching, continuous and aggravated during menstruation. There were no other associated symptoms. Obstetric history revealed that she was P2L2 with both deliveries being vaginal. Episiotomy was performed during both deliveries. Menstrual history was non-contributory other than aggravation of pain during menstruation in the perianal region. Her vitals were stable and systemic examination was normal. On local examination, a perianal abscess was seen at 8’o clock position. Surgical excision was done and resected specimen was sent for histopathological examination. Histopathology of the excised tissue showed endometrial glands of variable size within the endometrial stromal cells surrounded by dense fibrous tissue. Occasional hemosiderin laden macrophages were seen. [Fig. 1a, 1b & 2a] Immunohistochemistry (IHC) showed positivity for CD10, which is expressed in endometrial stromal cells. [Fig. 2b] The histomorphological and IHC findings support the diagnosis of endometriosis. The post operative course of the patient was uneventful.
 |
Click here to view |
Fig 1: (1a) Photomicrograph showing endometrial gland with cellular stroma surrounded by fibrosis, low power magnification. (100X, H&E stain), (1b) Photomicrograph showing endometrial glands surrounded by decidualised stroma, high power magnification. (400X, H&E stain)
 |
Click here to view |
Fig. 2: (2a) Photomicrograph showing a field with only endometrial stromal cells, high power magnification. (400X, H&E stain). (2b) Photomicrograph showing endometrial stromal cells diffuse positivity for CD10. (400X, IHC)
Scar endometriosis usually follows previous abdominal surgery, especially early hysterectomy and caesarean section. Minaglia et al. who analysed 30 years of incisional endometriosis after caesarean section found the incidence of scar endometriosis to be 0.08%.[5] Ectopic pregnancies, salpingectomy puerperal sterilization, laparoscopy, amniocentesis, appendectomy, episiotomy, vaginal hysterectomies, and hernia repair are the other surgical factors for scar endometriosis.[6],[7],[8]
There are various theories concerning the scar endometriosis. One of them is the direct implantation of the endometrial tissue in scars during the operation.[9] Under proper hormonal stimulus, these cells may proliferate (cellular transport theory) or the neighbourhood tissue may undergo metaplasia, which leads to scar endometriosis (coelomic metaplasia theory). By lymphatic or vascular pathways, the endometrial tissue may reach the surgical scar and then generate to scar endometriosis. Direct mechanical
implantation seems to be the most plausible theory for explaining scar endometriosis.[10]
Perianal endometriosis is a rare entity (0.2% of ectopic endometriosis) with only few cases reported.[11],[12]Perineum
is an unusual location for endometriosis, where it is
frequently confined to episiotomy scar, as a result of tissue implantation taking place during episiotomy procedure.[12] In this case swelling was present at episiotomy scar site.
Perianal swelling with cyclical pain and bleeding during menstruation may help in diagnosis of perianal endometriosis. It is rarely considered as one of the differential diagnosis of perianal problems by the clinicians as the characteristic cyclical pain is uncommon in perianal region.[2]
A recurrent painful perianal swelling with no pus, observed on drainage should arouse the suspicion of endometriosis. Fine needle aspiration cytology has shown to be beneficial in diagnosis, although biopsy of unusual lesion in patient with recurrent perianal pain is considered confirmative diagnosis.[2],[13]Histopathological examination shows presence of endometrial glands surrounded by endometrial stromal cells along with hemosiderin laden macrophages.[1],[2],[3]Immunohistochemically, CD10 is a sensitive and specific marker for endometrial stromal cells.[3],[4]CD10, also called common acute lymphoblastic leukaemia antigen (CALLA), is a neutral peptidase typically used in phenotyping of leukaemia and lymphoma. However CD10 is also being used in identifying normal, ectopic and neoplastic endometrial stromal cells,[3][4]as demonstrated in our case too. Thus it is very helpful in the confirmation of diagnosis.
Wide local excision is the surgical intervention of choice.[2]Same was done in our patient, sparing anal sphincter. The patient has shown no signs of recurrence even after lapse of 10 months following surgery at the time of writing this manuscript.
Conclusion
Endometriosis should be considered in differential diagnosis of painful perianal swellings in females particularly with a history of episiotomy. Biopsy is helpful in diagnosis. CD10 staining is of value in establishing a definitive diagnosis of endometriosis.
Conflicts of Interest: None.
How to cite : Kuchanur V, Kulkarni V, Bijjaragi S, Chandrasekhar H R, Rajashekar K S, Perianal endometriosis: A rare case report. IP Arch Cytol Histopathol Res 2019;4(1):99-101
This is an Open Access (OA) journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.