IP Archives of Cytology and Histopathology Research
Official Publication of Khyati Education and Research Foundation
Official Publication of Khyati Education and Research Foundation

Print ISSN: 2581-5725
Online ISSN: 2456-9267
CODEN : IACHCL
IP Archives of Cytology and Histopathology Research (ACHR) open access, peer-reviewed quarterly journal publishing since 2016 and is published under the Khyati Education and Research Foundation (KERF), is registered as a non-profit society (under the society registration act, 1860), Government of India with the vision of various accredited vocational courses in healthcare, education, paramedical, yoga, publication, teaching and research activity, with the aim of faster and better dissemination of knowledge, we will be publishing the article more...Null
Author Details :
Volume : 4, Issue : 1, Year : 2019
Article Page : 102-104
https://doi.org/10.18231/2456-9267.2019.0018

Abstract
A 55 year male patient presented with progressive growth over left lower eyelid measuring 1.5 x 1 cm. The local examination showed ulceroproliferative growth with irregular margins and everted edges. On histopathological examination diagnosed as basal cell carcinoma of lower eyelid. We are presenting this case for its clinical manifestations and histopathological findings.
Keywords: Eyelid tumor, Basal cell carcinoma, Pigment.
The prevalence of Basal Cell Carcinoma (BCC) is on rise and it is estimated that every year there is increase in cases by 10% and the lifetime risk or developing BCC is around 30%.[1][2]The various malignant tumours arising from eyelids were reported, BCC accounts for 80 -90% of all malignant lid tumours.[3] The tumours show high rate of recurrence which is mostly related to incomplete surgical resection and involves most of the eye socket and intracranial extension.[4],[5]Histopathological subtype plays an important role in progress of disease. In our case it showed nodular type of BCC. We have studied its clinical behavior and progress.
A 55 year old male farmer by occupation presented to plastic surgery unit with complaint of growth over left eyelid of 6 month duration. The growth was measuring 1.5x 1cm with irregular margins, everted edges. The base was formed by a dark brown exudate with areas of blackish incrustation. The surrounding periorbital area shows swelling and oedema. No evidence of any palpable neck nodes. Wide excision of lower lid swelling was done and tissue was sent for histopathology examination. We received the excised specimen of ulceroproliferative growth of lower eye lid totally measuring 2.2 x 1.8x 0.6cm. The growth measured 1.7x 1x 0.4 cm which was grey white, firm. Areas of focal hemorrhages and blackish discoloration was noted (Fig. 1). The surgical margins appear free from growth. Microscopy showed epithelial neoplasm invading deeper tissue (Fig. 2) The tumour was arranged in nodular pattern with islands strands and clusters with peripheral palisidation. (Fig. 3,4). The area of blackish pigmentation was noted. On histopathological the diagnosis was nodular basal cell carcinoma (Fig. 5). The patient underwent wide excision with reconstruction of the defect. On regular followup patient responded well to treatment.
 |
Click here to view |
Fig. 1: growth over left eyelid measuring 1.5x 1cm with irregular margins, everted edges.
 |
Click here to view |
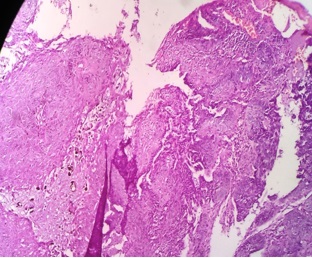
Fig. 2: microscopy showing ulcer and epithelial neoplasm invading deeper tissue. (Haematoxyline & Eosin stain, 40x)
 |
Click here to view |
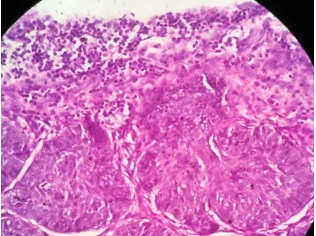
Fig. 3: microscopy showing the tumour arranged in nodular pattern with peripheral palisidation. (Haematoxyline & Eosin stain, 100x).
 |
Click here to view |
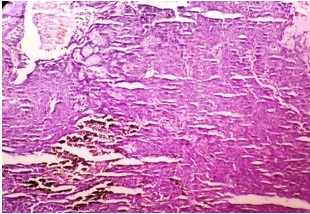
Fig. 4: microscopy showing the tumour arranged in nodular pattern with peripheral palisidation (Haematoxyline & Eosin stain, 40x).
 |
Click here to view |
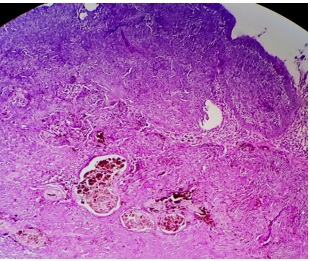
Fig. 5: microscopy showing the tumour arranged in nodular pattern with peripheral palisidation. The area of blackish pigmentation s noted. (Haematoxyline & Eosin stain,100x).
The most common malignant tumour of eyelid and surrounding structures are BCC 80-90%, followed by Squamous cell carcinoma – 40%, sebaceous carcinoma -5%, melanoma 1% etc.[2]
The common age affected were in elderly with highest incidence among patients of 70-75 years.[6]In our case patient was 55 years of age with involvement of lower eyelid. It is reported that lower lid is most commonly affected, site middle and upper lids are very rare to get involved. Various predisposing factors for basal cell carcinoma are albinism, xeroderma pigmentation, geographic, environmental and carcinogens have been explained[7] The farmers exposed to environmental risk factors are more likely to develop BCC at a younger age. On clinical presentation our patient showed irregular, ulceroproliferative growth with everted edges. The size is larger in our case as compared to other reported cases where size is 0.2-1.5 cm. Usually clinical presentation is of small papule which later on gives nodule formation, Associated with ulcer, pigmentation were noted
The definitive diagnosis is done on histopathological study. On histopathological examination our case showed diffuse, nodular, ulcerated lesion with classic palisidation of tumour and solid nodular growth pattern. Areas of melanin pigmentation was noted. The most common histological type of BCC is nodular (40-50%), other are infiltrative, (15 to 25%), ulcerative morphea like, sclerosing, mixed, basosquamous, pigmented etc.[2],[8] Rarely sebaceous differentiation was noted.
The treatment modalities are usually of surgical excision, local chemotherapy, cryotherapy, immune modulatory agents.[9]The high incidence of recurrence is noted if incomplete resection, involved resected surgical margin, location of tumour near canthus, infiltrative type at growth, morphea, basosquamous subtypes, high immunoreactive of ki 67 tumours. It is stated that surgical resection is good for the curative treatment. Rarely recurrence and metastasis have been noted. BCC a slowly progressive and poorly metastasizing skin cancer with propensity to be locally destructive Nature.[10],[11] The early diagnosis and adequate treatment is essential for better prognosis.
We are presenting this case for its clinical manifestations and histopathological findings. As the clinical feature, histopathological subtypes and treatment modality determines the coarse of disease.
Conflicts of Interest: None.
How to cite : Jagtap S V, Kumbhar S, Mane A, Kaur P, Wingkar C, Basal cell carcinoma of eyelid. IP Arch Cytol Histopathol Res 2019;4(1):102-104
This is an Open Access (OA) journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.