- Visibility 35 Views
- Downloads 7 Downloads
- DOI 10.18231/j.achr.2020.033
-
CrossMark

Adenomyomatous polyp – A culprit for infertility: rare case report
Introduction
Adenomyomatous polyp is a rare subtype of endometrial polyp in which smooth muscle is the prominent stromal component.[1] About 1.3% of endometrial polys are adenomyomatous polyps.[2] This lesion affects the females of fourth decade and later. Grossly it is very difficult to distinguish adenomyomatous polyp from ordinary endometrial polyp. [3], [4], [5] This polyp is comprised of smooth muscles, endometrial glands and endometrial stroma.[1]
There was no history of hormonal therapy. We report a case of 38-year female with history of secondary infertility.
Case Report
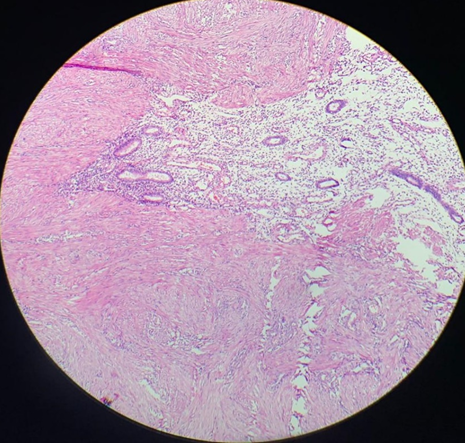
A 38 years female presented with a complaint of secondary infertility to the OPD at Adesh institute of medical sciences and research, Bathinda. There was no history of hormonal therapy. Hysteroscopy guided polypectomy under general anaesthesia was performed and the specimen was sent to the department of Pathology. On gross examination, a polypoidal grey white to tan tissue measuring 0.6x0.6x0.2cm was received. Hematoxylin stained slides examined show a polypoidal tissue lined by columnar to flattened lining epithelium. Subepithelium show small to elongated endometrial glands embedded in an edematous stroma. Intermixed are seen intersecting fascicles of smooth muscle fibres along with scattered blood vessels and chronic inflammatory infiltrate comprising of Lymphocytes, plasma cells and eosinophils. On histopathology Adenomyomatous polyp was the diagnosis ([Figure 1], [Figure 2]).

Discussion
Endometrial polyps of adenomyomatous type are rare. The origin is focal hyperplasia of basalis leading to the localized overgrowth of endometrial tissue containing variable amount of endometrial glands, stroma, smooth muscles and blood vessels. These polyps are sessile or pedunculated masses, single to multiple and vary in sizes from 0.5cm to 3 cm in diameter or may be larger.[6]
| Authors | Patient age | Hormonal therapy(tamoxifen) | Symptoms | Year of publication |
| Nasu et al 1 | 63 | Yes | None | 1997 |
| Fitzhugh et al 3 | 32 | No | Menometrorrhagia | 2008 |
| Takeuchi et al 9 | 64 | Yes | None | 2005 |
| Nasu et al 8 | 37-57 | No | Menorrhagia | 1995 |
| Sato et al 4 | 33 | No | None | 2007 |
| Silverberg SG 5 | 44 | No | Menorrhagia | 1975 |
| Huang et al 10 | 66 | No | Postmenopausal bleeding | 2017 |
| Babu et al 6 | 23 | No | None | 2012 |
| Bhagyalakshmi et al 7 | 25 | No | Menorrhagia | 2018 |
| Present case | 38 | No | Secondary infertility |
hows thatAdenomyomatous polyp usually seen in fourth decade and later in females which is in concordance to our case.
There is no history of any hormonal therapy in the present case that is similar to the studies of Fitzhugh et al,[3] Nasu et al, [8] Sato et al [4], Silverberg SG,[5] Huang et al,[9] Babu et al[6] and Bhagyalakshmi et al.[10] Only two authors Nasu et al,[1] and Takeuchi et al[7] have history of tamoxifen therapy.
The most common presenting symptom is the bleeding per vaginum either menorrhagia or post- menopausal bleeding (Fitzhugh et al [3], Nasu et al,[8] Silverberg SG [5], Huang et al [9] and Bhagyalakshmi et al. [10]) In the studies of Nasu et al,[1] Sato et al[4] and Babu et al[6] the patients were asymptomatic. Our case is unique in the way of presention as secondary infertility. To the best of our knowledge, no case of adenomyomatous polyp has ever been presented with the complaint of inability to conceive, in the literature.
About 1.3% of endometrial polys are adenomyomatous polyps.[2] Incidence of endometrial polyps is higher in women treated with tamoxifen (8 to 36 %) than in untreated women (0-10 %)[7]
Treatment modalities depends on the size of the polyp and symptoms. Polypectomy suffices in small, asymptomatic lesions while hysterectomy is mandatory for the larger one causing frustrating symptoms.
Conclusion
Adenomyomatous polyp of endometrium is a rare entity which could be a possible culprit for the infertility.
Source of Funding
None.
Conflict of Interest
None.
References
- K. Nasu, K. Arima, J. Yoshimatsu, I. Miyakawa. Adenomyomatous Polyp of the Uterus in a Patient Receiving Tamoxifen. Jpn J Clin Oncol 1997. [Google Scholar]
- W F Peterson, E R Novak. Endometrial Polyps. Obstet Gynecol 1956. [Google Scholar]
- V A Fitzhugh, G Murphy, D S Heller. Adenomyomatous polyp of the endometrium: a case report. J Reprod Med 2008. [Google Scholar]
- Hirokazu Sato, Hiroshi Nanjo, Hidenori Tanaka, Toshinobu Tanaka. Arias-Stella reaction in an adenomyomatous polyp of the uterus. Acta Obstet Gynecol Scand 2007. [Google Scholar]
- Steven G. Silverberg. Adenomyomatosis of Endometrium and Endocervix—A Hamartoma?. Am J Clin Pathol 1975. [Google Scholar]
- Y P Babu. Adenomyomatous polyp of the uterus: Report of an autopsy case and review of the literature. J Forensic legal med 2012. [Google Scholar]
- Bhagyalakshmi. Diffuse multiple giant adenomyomatous endometrial polyps- a rare case report. JNTR Uni Health Sci 2018. [Google Scholar]
- K. Nasu, T. Sugano, I. Miyakawa. Adenomyomatous polyp of the uterus. Int J Gynecol Obstet 1995. [Google Scholar]
- S M Ascher, J C Johnson, W A Barnes. MR imaging of the uterus in postmenopausal women receiving tamoxifen therapy for breast cancer: histopathological correlation. Radiol 1996. [Google Scholar]
- Ci Huang, Mun-Kun Hong, Dah-Ching Ding. Endometrial adenomyoma polyp caused postmenopausal bleeding mimicking uterine malignancy. Gynecol Minim Invasive Ther 2017. [Google Scholar]