
Introduction
Gallbladder cancer is the most common and highly lethal malignancy of the biliary tract worldwide. A very high incidence of this cancer is reported from North India. Primary squamous cell carcinoma (SCC) of the gallbladder is a rare entity that comprises between 1-3% of all primary GB cancers.1 Although areas of squamous differentiation are seen in adenocarcinoma, pure primary squamous cell carcinoma of gallbladder is rarely reported. There is a poorer prognosis associated with primary SCC of the gallbladder as compared to the more common Adenocarcinoma subtype as it is thought to be more locally invasive, and is often typically diagnosed at a more advanced T stage.2 SCC gallbladder is usually detected at an advanced stage with infiltration into adjacent structures, commonest site being the liver.
Ultrasound-guided fine-needle aspiration cytology is considered an important minimally invasive investigation in the preoperative diagnosis of carcinoma of the gallbladder.3 It is a safe, quick and precise diagnostic procedure for early diagnosis and management of gallbladder cancer in developing countries. However, cytologic descriptions of the diagnosis of the rare primary Squamous cell carcinoma of the gallbladder are sparse. Here we report two cases of squamous cell carcinoma of gall bladder diagnosed on ultrasound guided fine needle aspiration cytology leading to timely diagnosis and effective management.
Case Report
Hereby, we report two cases, one male and a female patient both of whom presented with symptoms of pain abdomen, vomiting without any history of weight loss or jaundice to the Surgery OPD of Hakeem Abdul Hameed Centenary Hospital (HAHC), New Delhi.
Case 1
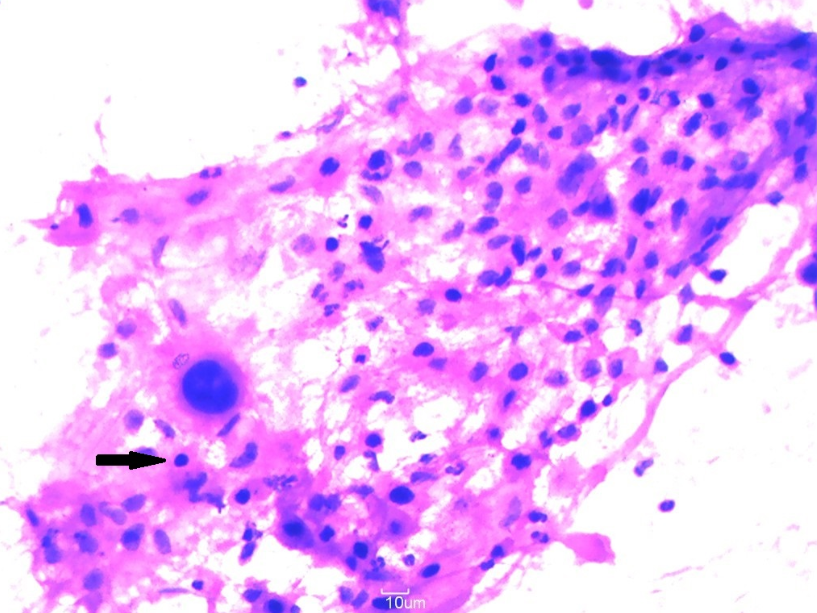
A 55 year female presented with a lump right upper abdomen and intermittent vomiting for 1 month. Examination revealed a hard, irregular mass in the right hypochondrium. Hematological parameters were within normal limits. Ultrasonography showed gallstone disease with localized thickening of the GB wall. On CT abdomen, a heterogenous lobulated mass was seen within gall bladder with wall thickening at fundus and contiguous infiltration of adjacent liver parenchyma. Without delay, a ultrasound guided FNAC was done which showed aggregates of atypical squamous cells with hyperchromatic nuclei, increased N:C ratio, abundant eosinophilic cytoplasm with occasional multinucleated giant cells and few inflammatory cells in the background. With these above findings the cytologic diagnosis of malignant lesion of gall bladder suggestive of Squamous cell carcinoma was given. (Figure 1 ) Extended cholecystectomy was done two weeks following the cytological diagnosis. On histopathology, a final diagnosis of pure Squamous cell carcinoma of gallbladder was made.
Case 2
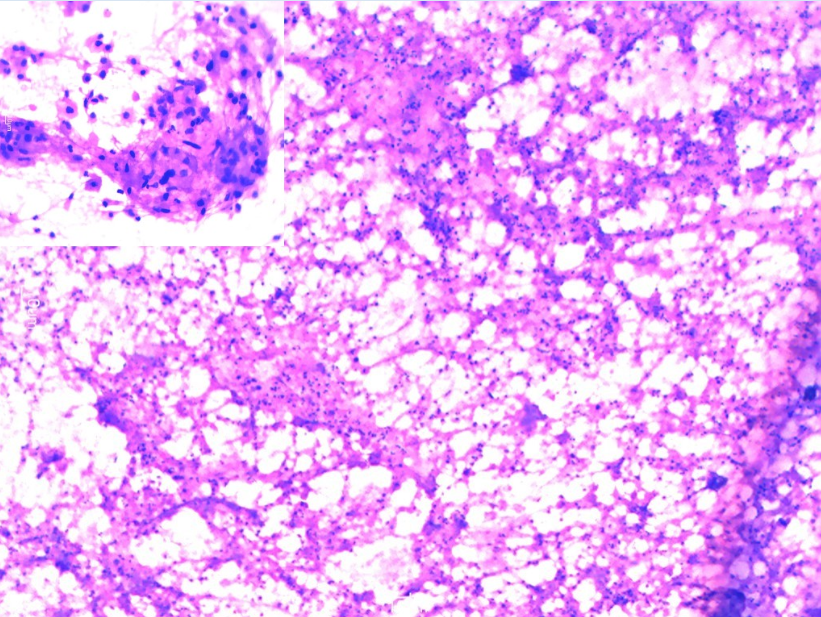
A 85 year male presented with pain upper abdomen and vomiting since one week. Examination revealed mild tenderness in right hypochondrium without any palpable lump. Routine investigations were within normal limits. Ultrasound revealed cholelithiasis with localized thickening at fundus of gallbladder. CT abdomen was reported as a neoplastic process involving the wall of gall bladder at fundus with extension into adjacent liver and retroperitoneal lymph nodes. USG guided FNA was done from gall bladder which showed small aggregates of atypical epithelial cells with enlarged hyperchromatic nuclei, moderate eosinophilic cytoplasm, irregular nuclear borders, seen against the background of abundant acute inflammatory cells. Few keratinized and tadpole cells with pyknotic nuclei were also seen along with keratinous debris. (Figure 2) With these features, cytological report suggestive of Squamous cell carcinoma of gall bladder was given. The patient refused any further treatment in the hospital and was lost to follow-up.
Discussion
Gallbladder diseases are very common with gallbladder carcinoma being the most common malignant tumor of the biliary tract. It predominates in the female population with variable prevalence in different parts of the world.4 The incidence is high in north and northeastern Indian population as compared to south India.5 This carcinoma is associated with poor prognosis which may be related to its aggressive behavior and also due to delayed diagnosis.
Adenocarcinoma is the most common histological subtype of gallbladder cancer constituting about 90-95% of the cases. Although areas of squamous differentiation are seen in some reported cases, pure squamous cell carcinoma of the gallbladder is very rare.6 The etiology and pathogenesis of squamous cell carcinoma is not well understood. Since there is no squamous lining in the gallbladder, SCC in the gallbladder may arise from heterotopic squamous epithelium, malignant transformation of metaplastic squamous epithelium or from squamous metaplasia of adenocarcinoma.7 SCCs usually behave aggressively with extension to liver and lack or rarity of lymph node involvement and no visceral metastasis.8
Image-guided FNAC plays an important role in diagnosis of gallbladder lesions with minimal complications. Cytologic diagnosis of gallbladder malignancies by FNA has become common due to accessibility of imaging techniques like ultrasound (US) and computed tomography (CT). Only few large studies on US/computed tomography guided percutaneous fine needle aspiration (FNA) of gallbladder are available in the literature until date with the diagnosis of SCC by FNAC being extremely rare.9 In a study of 82 cases of Ultrasound guided FNAC, Das et al described 12.5% cases of squamous and adenosquamous carcinomas.10 Although occasional studies have attempted to classify the gallbladder carcinoma on cytology, the literature search lacks the standardized cytological terminology and nomenclature system used for gallbladder lesions on FNAC.11
Pure squamous cell carcinomas of gallbladder are very rare. In a recent study by Chandra et al, it constituted 1.9%of the total malignant GB lesions.12 Roa et al. also observed only 1% of pure squamous cell carcinoma in a series of 34 squamous and adenosquamous carcinomas of the gallbladder.6 This carcinoma commonly extends to the liver and other neighboring structures and is diagnosed at advanced stage and thus has poor prognosis. The squamous cell carcinoma need to be associated with adenocarcinoma component for the diagnosis of adenosquamous carcinoma, but in our study in both the cases there was no adenocarcinoma component in all the smears examined.
Both the cases in our study did not reveal any symptoms of malignancy like weight loss, jaundice and were directly diagnosed on aspiration cytology. As the studies corroborates that squamous cell carcinoma of the gall bladder have poorer prognosis, early cytological diagnosis in our cases was imperative to the patients for early treatment. Thus, it is suggested that close cytological examination of smears is essential to precisely subtype the malignant tumors of the gallbladder which may thus be helpful in prognostication of these tumors.
Conclusion
Squamous cell carcinoma of gallbladder is a rare entity having worse prognosis. Even though a lot of new sophisticated imaging techniques have been developed, ultrasound guided cytological aspiration plays an important role in early pre-operative diagnosis and prognostication of squamous cell carcinoma of gall bladder thus contributing to early treatment in these patients.