
Introduction
Diarrheal illness can be associated with significant morbidity and mortality, especially in very young, elderly population and those with co morbid medical illness. Diarrhea can be classified based on the duration into acute, persistent and chronic. Chronic diarrhea is defined in adults by abnormal stool weight (>200 g/day), consistency (loose or liquid), and/or frequency (>3 times/day) lasting for more than 4 weeks.1, 2
The primary causes vary depending on socioeconomic factors, referral status as well as the practice setting. In developing countries chronic bacterial, mycobacterial infection, and parasitic infestation are the most common causes of chronic diarrhoea whereas in developed countries, irritable bowel syndrome, inflammatory bowel disease, malabsorption syndrome, and chronic infections are the most common causes.3, 4, 5, 6, 7 Colonoscopy has been used to evaluate the large bowel, to screen colorectal diseases especially neoplasia and polyps8, 4, 9 Colonoscopy visualizes the mucosa of the colon rectum and upto terminal ileum and checks for macroscopic lesions. Additionally, several procedures can be performed, especially biopsies.10, 11
Patients with chronic diarrhoea present a difficult diagnostic problem. Histology is essential in the evaluation of chronic diarrhoea, because many etiologies are macroscopically not evident e.g., quiescent inflammatory bowel disease (IBD), microscopic colitis, eosinophilic colitis and amyloidosis.1 In developing countries, most causes of chronic diarrhoea are non-infectious; include secretary diarrhoea, osmotic diarrhoea, fatty diarrhoea, inflammatory diarrhoea and functional diarrhea.12
This study was carried out with an aim to study the Histopathological patterns of colonic mucosal biopsies and correlate with clinical findings. Specimens were obtained from terminal ileum, colon and rectum, in inflammatory and neoplastic disorders. The histopathological findings of each lesion was worked up for chronic diarrhea.
Materials and Methods
The present prospective study was done in the Department of Pathology, Vydehi Institue of Medical Sciences and Research Centre, Bangalore, during a period of 1 year from January 2014 and January 2015. A total of 100 colonoscopic biopsies from the patients who presented with chronic diarrhea attending Gastro intestinal department were studied. During the procedure, gross pathology was noted and biopsies were taken from representative areas. Relevant clinical details and colonoscopic findings were taken for the study. The Histological diagnosis was given after the studying the haematoxylin and eosin (H&E) stained section. Special stain like Ziehl-Neelsen (ZN) was done to identify acid fast bacilli, to confirm the diagnosis of tuberculoses colitis.
Results
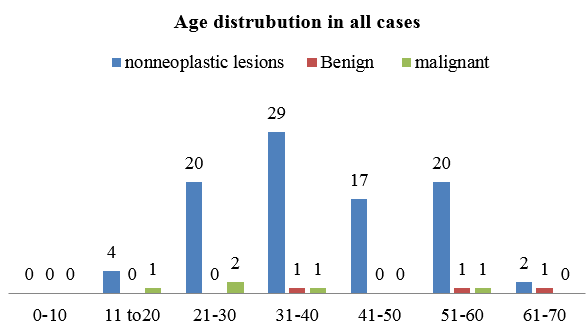
A total of hundred, colonoscopic biopsy were performed on age groups of patients ranged from 11 - 70years who had presented with features of chronic diarrhea. The majority of cases were males 77%(n=77) and females constituted 23% (n = 23) in the study population depicted in the (Table 1) with the male predominance of age group 31-40 years (31%) and minimum age of 61-70 years depicted in (Figure 1).
Table 1
Sex distribution of all case
|
Sex |
No. of patients |
% |
|
Male |
77 |
77.0 |
|
Female |
23 |
23.0 |
|
Total |
100 |
100.0 |
All 100 cases presented with the symptom of diarrhoea (seen in 100% of patients) and with other associated features like pain abdomen (37%), weight loss (8%), fatigue (24%).
Among the study patients the colonoscopic findings reported were mucosal erythema (18%) mucosal ulceration (50%) polyps (12%) and presence of mass lesion (5%). Normal mucosal study from patient subset was reported in 36(36%) of patients. Findings were mainly seen with male predominance. (Table 2) Among all the colonoscopic biopsies histologically 92 cases were diagnosed as non neoplastic and 8 cases of were diagnosed as neoplastic lesions.
Histopathological findings
On the basis of microscopic findings evaluated for chronic diarrhea of nonneoplastic lesions show mucosal ulceration 50% of patients could be wide range of diagnosis between inflammatory disease, neoplastic infections. With other features are specific to inflammatory bowel disease like cryptitis 28% and crypt abscess 25% were seen in patients respectively. architectural distortions was noted upto 19% of the patient inflammatory disease. Presence of granuloma which could be seen in tuberculosis colitis and crohns colitis 17% however the features of submucosal inflammatory infiltration and odema which could be differential diagnosis of nonspecific colitis, 11% ulcerative colitis 9% and crohns disease 5%. Non neoplastic lesions were found in all age group of 11 to 70 years with male to female ratio 3.3:1 (Table 2 and Figure 2)
Table 2
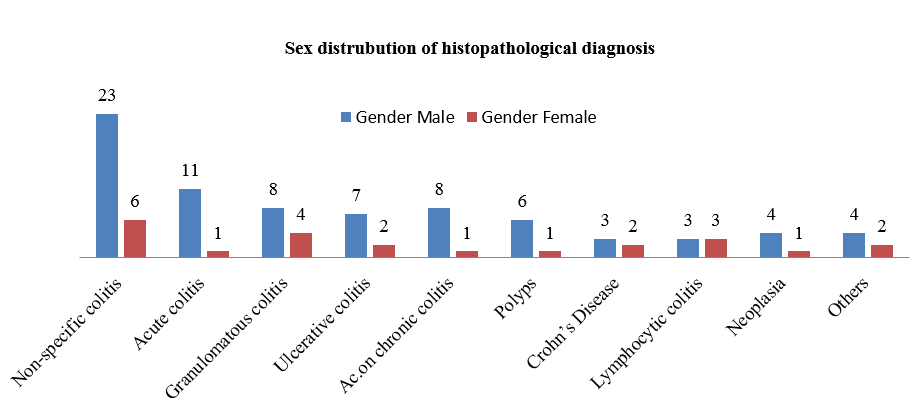
Sex distribution of Histopathological findings of patients studied
Among the total 100 cases 50% of cases were correlated with colonoscopy giving specific diagnosis on microscopy. The other 50% of cases were given as acute on chronic colitis, acute and chronic non-specific colitis, granulomatous colitis.
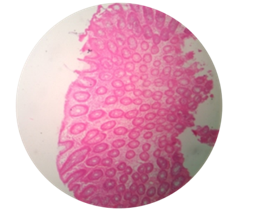
Figure 2
Photomicrograph of granulomatous colitis multiple pale pink granulomas H&EX10; b: Photomicrograph of granulomatous colitis multiple pale pink granuloma in sub mucosa H&EX40
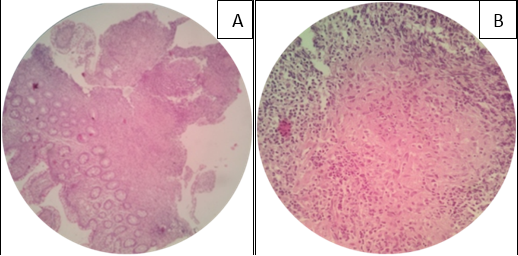
Figure 3
Photomicrograph of Ulcerative colitis, showing full thickness inflammation and cryptitis H&EX10
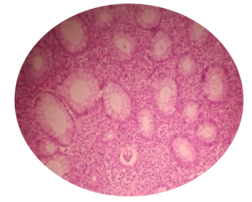
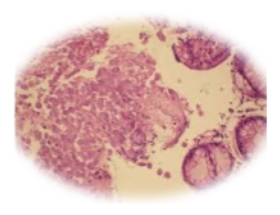
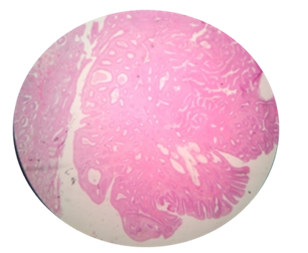
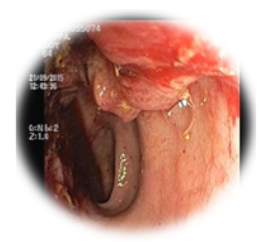

Table 3
Comparison of colonoscopic findings with different studies
|
Study |
No of cases |
Normal mucosa (%) |
Abnormal mucosa (%) |
|
Shah et al 5 |
168 |
60 |
40 |
|
Villafuerte-Galvez J et al 3 |
162 |
85 |
15 |
|
Present study |
100 |
36 |
64 |
Table 4
Comparison of Histopathological diagnosis with similar studies
|
Diagnosis |
Shah et al 11 |
Villafuerte G J et al 3 |
Lee JH et al 13 |
Present study |
|
No of cases |
168 |
162 |
118 |
100 |
|
Normal histology |
101 (60%) |
24 (14.8%) |
- |
- |
|
Non specific colitis |
15 (8.9%) |
|
93 (78.8%) |
29 (29%) |
|
Active & chronic active colitis |
3 |
6(3.7%) |
- |
21(21%) |
|
Tuberculous colitis |
- |
7 (4.3%) |
- |
12(12%) |
|
Ulcerative colitis |
7 |
4 (2.5%) |
1(0.8%) |
9 (9%) |
|
Polyps |
1 |
- |
- |
7 (7%) |
|
Crohn’s disease |
9 |
- |
- |
5 (5%) |
|
Lymphocytic colitis |
10 |
58 (35.8%) |
1 & 8 cases of some features of Lymphocytic colitis (7.8%) |
6(6%) |
|
Neoplasia |
- |
4 (2.5%) |
Exclusion |
5 (5%) |
|
Collagenous colitis |
Nil |
Nil |
2 & 8 cases of possible collagenous (8.5%) |
Nil |
|
Melanosis coli |
6 |
- |
4(3.4%) |
- |
|
Others |
16 |
8 (4.9%) |
- |
6 (6%) |
Histopathology of non neoplastic lesions
In the present study out of total 92 cases of non-neoplastic lesions, 85 cases were inflammatory lesions, 4 cases were polypoid lesions, 2 cases of lymphoid hyperplasia and 1 case was of amebic colitis. Among 85 cases of inflammatory lesions, 29 cases (34.1%) were chronic non-specific colitis, charcterised by increased lympho-plasmacytic infiltrate in the lamina propria with well-maintained crypt architecture and goblet cells with male predominance (Figure 3), where as specific diagnosis of 12 cases each of acute non-specific colitis (14.1%) cases showed neutrophilic infiltrates in the lamina propria along with cryptitis or crypt abscesses. Tuberculous granulomatous colitis were seen in 12 cases (14.1%) characterised by large areas of caseous necrosis with granulomas, langhans type of giant cells collared by lymphocytes and plasma cells. (Figure 4 a&b)
Ulcerative colitis was seen in 9(10.6%) cases of which 6(66.7%) were given as active phase with features of crypt architectural distortion, neutrophilic cryptitis, abscesses and basal lympho-plasmacytosis and mucosal ulceration (Figure 5) and 3 cases were in the resolving phase (33.3%) One case showed low grade dysplasia. 5 cases of Crohns disease showed histologically by well-maintained crypt architecture and preserved goblet cell population. The lamina propria showed lympho-plasmacytic infiltration along with ill-formed small granulomas. 3 cases of eosinophilic colitis showing eosinophils of 5-6/ HPF along with eosinophilic cryptitis and abscesses.
7 cases of polypoid lesions were diagnosed of which 3 cases were nonneoplastic, 1 case of hamartomatous The lesions were 1 inflammatory polyp, characterized by polyp lined with colonic mucosa and the lamina propria showed increased chronic inflammatory cell infiltration, and 2 cases of hyperplastic polyps, characterized by crenated or serrated appearance of elongated crypts Among all non-neoplastic lesions male predominane is noted One case of amoebic colitis was diagnosed, showed mucosal ulceration and normal crypt architecture. The lamina propria showed chronic inflammatory cells like lymphocytes, plasma cells, histiocytes along with many trophozoites.(Figure 6)
Histopathology of neoplastic lesions
Among 8 cases of neoplastic lesions, of which 3 were benign (37.5%) and 5 were malignant (62.5%). The three benign lesions were tubular adenomas (Figure 7) seen in our study were characterized by increased number of tubular glands in the lamina propria. Out of the five malignant lesions, 3 cases were adenocarcinomas (60%), one was mucinous adenocarcinoma and onecase of sigent ring cell carcinoma characterized by intracellular mucin pushing the nucleus to periphery to form signet ring cells.
Discussion
The present study fallowed the definition of chronic diarrhea given by ASGE guidelines,1 and also fallowed by Navneeethan U et al,5 Schiller LR et al,14 who considered the duration of symptoms to define chronic diarrhea. Patients presented with symptoms of diarrhea for more than 4 weeks, they were followed by colonoscopy, biopsy with histopathological examination.
The male patients were effected more 77(77%) than the 23(23%) females showing a male to female ratio of 3.3:1, age ranged from 11 to 70 years, youngest and oldest being male. The majority of patients were in the age group of 31-40 years (31%). This observation indicates that colonoscopy is a safe procedure done in all age groups and can be biopsied for further evaluation. The sex and age incidence were in concordance with studies done by Shah et al11 & Galvez V J et al.3
All the 100 cases were presented with diarrhea (bloody and non-bloody) along with other coexisting symptoms like pain abdomen (37%), weight loss (24%) and fatigue (8%), while the study done by Shah et al11 showed associated findings like pain abdomen (43%), weight loss (9%), rectal bleeding (27%) and anaemia (15%).
Among the patients evaluated by colonoscopic biopsies, 64% showed abnormal mucosa (Figure 8, Figure 9) and others were showing normal mucosa. The abnormal macroscopic findings reported were ulceration (50%), mucosal erythema, polyps and mass, Findings were comparable to retrospective study done by Shah et al11 and Galvez V J et al3 reported normal mucosa in 60% among 168 patients and 85.8% among 162 patients biopsied respectively In their study, they reported ulceration, elevated lesions and mixed lesions as abnormal colonoscopic findings. [Table 3]
In the present study among the non neoplastic lseions, non Specific colitis (29%) found to be the commonest lesion and studies done by Lee JH et al13 Talbot and Price12 showed same findings.
The present study reported 12 cases as tuberculosis commonest granulomatous lesion in India having male to female ratio of 2:1 mostly occurring at 40-60 years age group. The findings are akin to the studies done by Villa fuerte G J et al3 Pulimood A et al15 and Kirsch R et al.16
Ulcerative colitis though rare is emerging disease in India this condition portrays remission and relapses. In the present study, 9 cases of UC were diagnosed with a male to female ratio of 2:1 and occurring at the age group of 20-40 years which are comparable to done by Deroche et al,17 Shah et al11 described 7 cases of ulcerative colitis in their colonoscopic study of 168 cases.
Cornhs diseases were seen in 5 cases in present study with a male to female ratio of 1.5:1 the findings are similar to Pulimood A et al15 and Shah et al11 gave the average age at onset as 33.3 years and male to female ratio as 1.5:1.
In the present study, there were 21 cases reported as chronic active colitis with male predominance (8:1). All cases showed infiltration with both chronic and acute inflammatory cells. Similar histopathological findings were seen in Preiser F et al18 and De Roche TC et al.17
In the present study, there were 3 cases of eosinophilic colitis showing eosinophils of 5-6/ HPF along with eosinophilic cryptitis and abscesses. Shah et al11 in their study of 168 patients, 1 case was diagnosed as eosinophilic colitis.
In the present study 1 case was diagnosed as amoebic colitis, characterized by many trophozoites along with chronic inflammatory cell infiltration in the lamina propria. Eosinophilic colitis, lymphoid hyperplasia and amoebic colitis were included in the present study. 79 Galvez JV et al3 studied 162 patients, which included solitary rectal ulcer, colonic spirochetosis, colonic histoplasmosis, eosinophilic colitis and pseudomembranous colitis as others.
Benign lesions
All the 3 neoplastic polyps were benign seen in males and are tubular adenomas with the age range of 40-60 years Chopra S et al19 studied biopsies of colorectal polyps in 2 phases, the second phase to determine incidence among 100 polyps 34 cases were tubular adenomas occurring at the average age of 62.5 years having equal incidence in males and females.
Malignant lesions
In the present study, there were 5 cases of neoplasia diagnosed in the age group of 30-50 years with male predominance. Most common sub type were adenocarcinomas, 1 case of mucinous adenocarcinoma showing extracellular mucin along with neoplastic cells and 1 case of signet ring cell carcinoma. Similar findings are seen with Galvez JV et al3 4 cases (2.5%) were reported as neoplastic in which the histological diagnoses given were adenocarcinoma, lymphoma and signet ring cell carcinoma.
Conclusion
Endoscopic evaluation of the large bowel has been greatly enhanced by the availability of flexible colonoscopies. A variety of non-neoplastic and neoplastic features were reported in the present study across a wide age distribution and findings correlated with that of similar studies. A greater awareness of the disease and understanding of pathogenesis on the part of the pathologist was felt to be necessary for a better and relevant reported diagnosis.
Hence, colonoscopic biopsies have increased the role of pathologists in the diagnosis and management of patients with chronic diarrhea so that proper clinico-pathological correlation can be made to assess severity and to guide treatment accordingly.