- Visibility 62 Views
- Downloads 11 Downloads
- DOI 10.18231/j.achr.2021.040
-
CrossMark

Histopathological array of cardiac lesions: An autopsy based study in a tertiary care centre
- Author Details:
-
 Renuka Verma *
Renuka Verma *
-
Sunita Singh
-
Nisha Marwah
-
Richa Pawar
-
Deepshikha Rana
Introduction
Cardiovascular diseases (CVD) are the leading cause of death worldwide with an incidence of 60-70%.[1] At the turn of century, it has became the leading cause of morbidity in India because of increase in cardiovascular risk factors. In 2016, the estimated prevalence of CVD in India was estimated to be 54.5 million. A quarter of all mortality is attributable to CVD. Ischemic heart disease and stroke are the predominant causes and are responsible for >80% of CVD deaths.[2] These diseases tend to affect patients in the most productive years of their lives and result in catastrophic social and economic consequences.
There is no valid method for sampling living population also there is moderate concordance between clinical and pathological causes of death. Over one fifth of clinically unexpected autopsy findings are correctly diagnosed only by histological examination. Autopsy and particularly autopsy histology are still the most accurate method of determining the cause of death and auditing accuracy of clinical diagnosis, diagnostic tests and death certification. It can also help in studying epidemiological profile, patho-physiology and management modalities of various cardiac lesions.[3]
Against this background, to assess the magnitude of problem, this study was done to determine the cause and nature of cardiac death and to observe various histo-morphological changes including 1000 autopsy specimens of whole heart.
Materials and Methods
The present retrospective randomized study was conducted in the Department of Pathology, Pt.B.D.Sharma, PGIMS, Rohtak, Haryana over the period of 9 months.
Case selection
A total of 1152 autopsies submitted to this institute for post-mortem examination, irrespective of cause of death, were analysed. The cases were medico legal and involved individuals of all age-group, sex, religion and caste. Epidemiological data and post mortem findings were noted from the post mortem and police papers.
Exclusion criteria
Out of total 1152 autopsies, specimen of heart was included in 1062 autopsies, out of which 62 were ill preserved and completely autolysed and were excluded from the study. Hence, 1000 whole heart specimens were included in our study.
Gross examination of heart
The samples were received in 10% formalin fixative with brief history and clinical details. The heart specimens were measured, weighed and examined externally for any rupture, infarct and discoloration. The heart was then dissected by modified Virchow’s method following the direction of blood flow.[4] All the chambers were washed off any blood clots and were examined for any pathology of valves including stenosis or calcification and endocardium for vegetations or thrombi. Thickness of ventricular walls and inter-ventricular septum was measured. Areas of myocardial ischaemia were serial sectioned and noted for their location and size. The three main vessels including right coronary artery (RCA), left circumflex artery (LCA) and left anterior descending artery (LAD) were examined using sections at regular intervals of 4-5 mm for any hardening, blockage and plaque. The aorta was checked for any dilatation, thickening and plaque.
Microscopic examination
Representative sections were taken from right and left ventricular wall, atrio-ventricular junction, inter ventricular septum, apex, three coronary arteries, valves and stump of aorta. Additional sections were taken from suspected pathological lesions. The sections were routinely processed and stained with Haematoxylin and Eosin stain for microscopic examination.[5], [6] pecial stains including Van Gieson, Masson Trichrome and Von Kossa were applied according to need and nature of lesion. The microscopic findings were noted and were correlated clinically.
Statistical analysis
The results of the study were statistically analyzed using the Statistical Package for the Social Sciences (SPSS) version 20 (IBM Corp. SPSS statistics, in Armonk NY) for windows. Data were expressed as mean±standard deviation and range for quantitative variables, numbers, and percentage.
Results
A total of 1152 autopsies received in the department of pathology were analysed. Out of these 90 cases did not include heart tissue and 62 cases were autolysed to yield any findings and were excluded from the study. Hence, a total of 1000 specimen of whole heart were included in our study.
Age and sex distribution
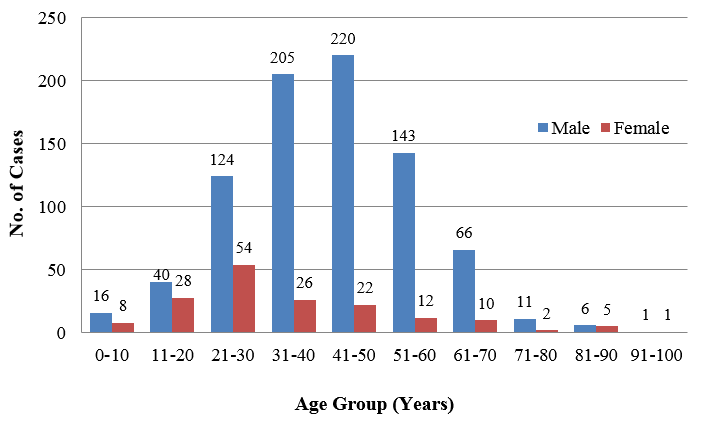
All the cases were divided into age groups based on the age at the time of death. The youngest case was newborn female and the oldest was 96 years male forming a age range of 0-96 years. Mean age was 42.64 years. Mean age for males was 40.65 years and for females was 36.13 years. Maximum number of cases presented in the age group of 41-50 years i.e. 242 (24.2%).
Out of 1000 cases, 832 (83.2%) were males and 168 (16.8%) were females forming a ratio of 4:95. There was remarkable male dominance. The age and sex distribution are shown in.[Figure 1]
Weight distribution
The post fixation heart weight ranged from 20 gm to 680 gm in males and 20 gm to 530 gm in females. The mean weight of the heart was 293.73 gm. Mean weight of heart for males was determined to be 302.08 gm and for females was 241.43 gm. ([Table 1])
Clinical details
The cases presented with variable cause of death. Majority of them (36.3%) had cardiovascular symptoms like chest pain, breathlessness and dizziness. Second most common cause was unknown previous illness (11%) and cases were under treatment. 10% cases were brought dead following collapse or an uncommon preceding event. ([Table 2])
Histopathological changes in heart
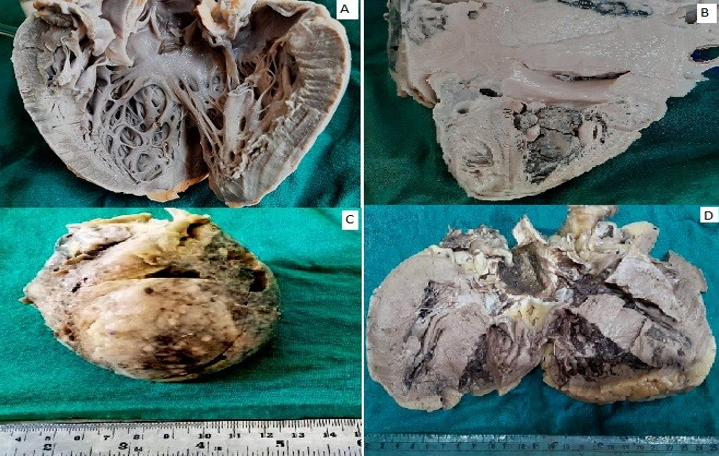
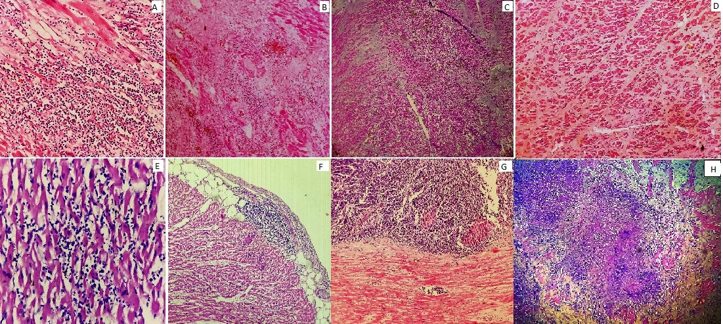
A wide spectrum of histopathological changes were observed on microscopic examination. Coronary atherosclerosis (CA) was the most common finding seen in 610 cases, followed by ischaemic heart disease (IHD) in 346 cases. 27 cases showed pericarditis, myocardial hypertrophy was found in 23 cases, 16 cases revealed myocarditis, 11 cases had ventricular haemorrhage due to trauma, 8 cases had changes of electrocution, 7 cases showed tuberculosis with variable involvement of pericardium and myocardium, 6 cases had calcification of valve and 4 cases revealed metastasis from carcinoma. In 304 cases (30.4%), no significant pathological changes were noted in heart. ([Figure 2], [Figure 3] and [Table 3])
One case each of rheumatic heart disease (at 14 year of age) and infective endocarditis (at 35 year of age) were also noted. In age group 0-10 years microscopic examination of heart and vessels was unremarkable. No congenital anomaly was seen in newborn and infants heart.
Changes in coronary arteries
Overall prevalence of atherosclerosis was 61.0%. In our study there was no case in age less than 10 years and there was significant increase in number and severity of atherosclerosis after third decades. All the cases with age more than 70 years had significant atherosclerosis
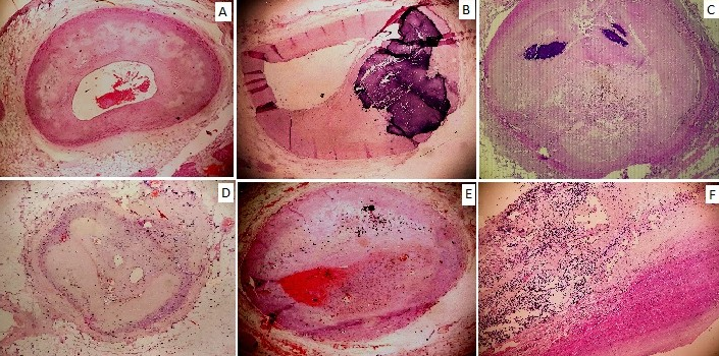
Out of the three coronary arteries, left anterior descending (LAD) was most commonly involved vessel (436 cases), followed by left circumflex artery (LCA) (416 cases) and right coronary artery (RCA) (393 cases). Secondary changes in coronary arteries like calcification, thrombus formation and plaque rupture were seen in 130, 97, 86 cases of LAD, LCA and RCA respectively. ([Figure 4] and [Table 4])
Complete occlusion of vessel was seen in 16, 12, 4 cases of LAD, LCA and RCA respectively. In 152 cases (24.4%) aorta also showed atherosclerotic plaques. One case of aortitis was also noted. The clacification was confirmed by Von kossa stain and disrupted elastic fibres were demonstrated by Von geison stain. Most of the cases (51.62 %) revealed triple vessel disease followed by double vessel disease (32.14%) and single vessel disease (16.24%).
Pattern and distribution of IHD
Overall prevalence of IHD was 34.6% with features of chronic IHD (CIHD) in 21.6%, acute myocardial infarction (AMI) in 8.5% and acute on chronic IHD in 4.5%. A significant association was found between increasing age and incidence of IHD, with maximum number of cases reported in the age group of 51-60 years.
The most common pattern of involvement was diffuse i.e. involvement of all the areas including left ventricular wall (LVW), inter ventricular septum (IVS) and apex (37.57%), followed by isolated involvement of left ventricular wall (22.83%). Isolated involvement of right ventricular wall (RVW) was seen in one case of acute MI. ([Table 5])
|
Heart Weight (gm) |
Male |
Female |
Total (%) |
|
0-50 |
10 |
05 |
15(1.5) |
|
51-100 |
06 |
03 |
09(0.9) |
|
101-150 |
12 |
04 |
16(1.6) |
|
151-200 |
64 |
27 |
91(9.1) |
|
201-250 |
115 |
50 |
165(16.5) |
|
251-300 |
250 |
42 |
292(29.2) |
|
301-350 |
181 |
20 |
201(20.1) |
|
351-400 |
120 |
10 |
130(13.0) |
|
401-450 |
42 |
04 |
46(4.6) |
|
451-500 |
15 |
02 |
17(1.7) |
|
501-550 |
08 |
01 |
0 (0.9) |
|
551-600 |
05 |
00 |
05(0.5) |
|
601-650 |
03 |
00 |
03(0.3) |
|
651-700 |
01 |
00 |
01(0.1) |
|
Total |
832 |
168 |
1000(100) |
|
S.No. |
Cause of death |
No. of cases |
Percentage |
|
1. |
Cardiovascular symptoms |
363 |
36.3 |
|
2. |
Unknown illness |
110 |
11.0 |
|
3. |
Brought dead |
100 |
10.0 |
|
4. |
Sudden & natural death |
79 |
7.9 |
|
5. |
Poisoning |
68 |
6.8 |
|
6. |
Road side accident |
47 |
4.7 |
|
7. |
Respiratory symptoms, Tuberculosis |
40 |
4.0 |
|
8. |
GIT symptoms |
26 |
2.6 |
|
9. |
Alcohol intoxication |
24 |
2.4 |
|
10. |
Drowning |
23 |
2.3 |
|
11. |
Death due to cold |
22 |
2.2 |
|
12. |
Electrocution |
20 |
2.0 |
|
13. |
Post-partum illness |
16 |
1.6 |
|
14. |
Hanging |
15 |
1.5 |
|
15. |
Homicide |
12 |
1.2 |
|
16. |
Snake bite |
09 |
0.9 |
|
17. |
Fall from height |
08 |
0.8 |
|
18. |
Starvation |
07 |
0.7 |
|
19. |
Seizures |
05 |
0.5 |
|
20. |
Burns |
04 |
0.4 |
|
21. |
Still birth |
02 |
0.2 |
|
|
Total |
1000 |
100 |
|
Age (Years) |
Normal |
CA |
CIHD |
AMI |
Acute on CIHD |
HCMP |
Myo-carditis |
Peri-carditis |
Electrocution |
Calc. of valve |
TB |
Vent H’ghe |
Mets |
|
0-10 |
24 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
|
11-20 |
58 |
2 |
0 |
0 |
0 |
3 |
3 |
2 |
0 |
0 |
0 |
0 |
0 |
|
21-30 |
86 |
70 |
10 |
14 |
4 |
5 |
3 |
6 |
2 |
0 |
2 |
4 |
0 |
|
31-40 |
70 |
134 |
46 |
16 |
6 |
5 |
4 |
7 |
3 |
0 |
3 |
3 |
0 |
|
41-50 |
46 |
181 |
50 |
20 |
8 |
6 |
2 |
5 |
2 |
1 |
1 |
3 |
1 |
|
51-60 |
16 |
128 |
52 |
22 |
10 |
3 |
3 |
4 |
1 |
1 |
1 |
1 |
2 |
|
61-70 |
4 |
69 |
44 |
10 |
12 |
1 |
1 |
2 |
0 |
2 |
0 |
0 |
0 |
|
71-80 |
0 |
13 |
7 |
2 |
3 |
0 |
0 |
0 |
0 |
1 |
0 |
0 |
0 |
|
81-90 |
0 |
11 |
5 |
1 |
2 |
0 |
0 |
1 |
0 |
1 |
0 |
0 |
1 |
|
91-100 |
0 |
2 |
2 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
|
Total |
304 |
610 |
216 |
85 |
45 |
23 |
16 |
27 |
8 |
6 |
7 |
11 |
4 |
|
Coronary artery |
Atherosclerosis |
Complications |
Total |
||||
|
Mild |
Moderate |
Severe |
Calcification |
Thrombus |
Plaque rupture |
||
|
RCA |
113 |
122 |
72 |
83 |
3 |
0 |
393 |
|
LCA |
121 |
128 |
70 |
90 |
6 |
1 |
416 |
|
LAD |
102 |
106 |
98 |
112 |
16 |
2 |
436 |
|
Total |
336 |
356 |
240 |
285 |
25 |
3 |
1245 |
|
Walls affected |
Chronic IHD |
Acute MI |
Acute on chronic IHD |
Total (%) |
|
Only RVW |
0 |
1 |
0 |
1(0.29) |
|
Only LVW |
50 |
19 |
10 |
79(22.83) |
|
Only IVS |
16 |
3 |
0 |
19(5.49) |
|
LVW and IVS |
18 |
5 |
2 |
25(7.22) |
|
Apex |
33 |
16 |
6 |
55(15.90) |
|
Apex and IVS |
21 |
8 |
8 |
37(10.70) |
|
All |
78 |
33 |
19 |
130(37.57) |
|
Total |
216 |
85 |
45 |
346(100) |
Discussion
Histopathological examination of heart plays an important role in determining whether death is attributable to a cardiac disease or to other cause, to determine the nature of cardiac disease, whether the mechanism was mechanical or arrhythmic and to rule out the possibility of trauma or any other unnatural cause.[7]
Out of 1000 whole heart specimens from our study, 83.2% were males and 16.8% were females, indicating that death from all causes including cardiac and non-cardiac was more common in men, and most of the cardiovascular deaths occurred within the age range of 41-60 years. This may be due to westernization of Indian society, sedentary life style, poor diet habits and lack of regular medical checkups. Secondly, there is increased indulgence to smoking and alcohol in males, while in females, estrogen has vasoprotective effects. These findings are supported by many studies showing similar male predominance and role of increasing age in sudden cardiac death patients with Karnafil R et al having maximum case in 41-50 years age range, Rao D et al in 50-60 years and Chug SS et al in 50-59 years.[8], [9], [10]
We also observed that in adolescents and young adults (<40 years) hypertrophic cardiomyopathy, myocarditis, pericarditis, tuberculosis, electrocution, ventricular haemorrhage due to trauma and premature coronary artery disease were found to be a major causative factor. While after 40 years, coronary atherosclerosis and IHD were predominant findings along with metastasis and calcification of valve in a few cases. These findings are in concordance with study done by Rao D et al, Singh P et al and Marwah et al.[9], [11], [12]
In this study, the prevalence of coronary atherosclerosis was 61.0%, which is comparable to other studies done by Shah SN et al (61.18%), Garg S et al (55.3%) and Joshi C et al (64%).[13], [14], [15] In terms of frequency of involvement and secondary changes LAD was most commonly involved vessel, followed by LCA and RCA. These findings are in concordance with studies done by Shah SN et al with LAD as most frequently involved vessel (38.70%) followed by LCA (36.56%) and RCA (31.18%). However, secondary changes were more commonly seen in LCA followed by LAD and RCA.[13]
Triple vessel involvement was most common in our study (51.62 %) followed by double and single vessel involvement 32.14% & 16.24% respectively. It was correlated with the study done by Porwal et al with triple vessel involvement in 40%, double vessel in 37% and single vessel in 15% case.[16] It was supported by Garg M et al who also reported triple vessels as the most commonly involved vessels (44.4%).[17] However, Virmani et al showed single vessel involvement as most commonly involved vessels (44%).[18]
In our study, nearly all cases with ischaemic heart disease had variable degree of atherosclerosis as reported by Marwah N et al.[11] In terms of frequency distribution of various areas, diffuse involvement of all the areas was most common pattern (37.57%), followed by involvement of left ventricular wall (22.83%) and apex (15.90%). Isolated involvement of RVW was seen in one case of acute MI. These findings are in accordance to those well documented in literature.[13], [19]
Conclusion
To conclude, in this study, ischemic heart disease with coronary artery atherosclerosis was found to be the leading cause of death with triple vessel disease as the most common pattern of involvement. Autopsy is the first and last opportunity to make an accurate diagnosis. The autopsy report should relate the pathological findings to the clinical history including circumstances of death and any other investigation performed close to the time of death.
Conflict of Interest
The authors declare that there are no conflicts of interest in this paper.
Source of Funding
None.
References
- R Matoba, I Shikata, K Iwai, S Onishi, N Fujitani, K Yoshida. An epidemiologic and histo-pathological study of sudden cardiac death in Osaka Medical Examiner's office. Jpn Circ J 1989. [Google Scholar]
- . India State-Level Disease Burden Initiative CVD Collaborators. The changing patterns of cardiovascular diseases and their risk factors in the states of India: the Global Burden of Disease Study 1990–2016. 2018. [Google Scholar]
- S Tyagi, R B Sukhadeve, H M Pathak. Autopsy Findings in Sudden Cardiac Deaths: Study in Medicolegal Autopsies. Sch J App Med Sci 2016. [Google Scholar]
- DE William, L Jurgen. Cardiovascular System. Handbook of Autopsy Practice. 3rd Edn. 2002. [Google Scholar]
- TS Lena, DB John, H Michael. Tissue Processing. Theory and Practice of Histological Techniques. 6th Edn. 2011. [Google Scholar]
- G Marilyn, H Michael. The Hematoxylins and Eosin. Theory and Practice of Histological Techniques, 6th edn . [Google Scholar]
- C Basso, B Aguilera, J Banner, S Cohle, G Amati, RS De Gouveia. Guidelines for autopsy investigation of sudden cardiac death: 2017 update from the Association for European Cardiovascular Pathology. Virchows Arch 2017. [Google Scholar]
- R Karanfil, M K Gulmen, A Hilal. Evaluation of cardiac conduction system in sudden death cases. J For Med 2013. [Google Scholar]
- D Rao, D Sood, P Pathak, S D Dongre. Cause of sudden cardiac deaths on autopsy findings; a four-year report. Emergency 2014. [Google Scholar]
- SS Chugh, KL Kelly, JL Titus. Sudden cardiac death with apparently normal heart. Circulation 2000. [Google Scholar] [Crossref]
- P Singh, R N Satarkar, S Kalhan, S Hasija, Bhawna, A Sangwaiya. Correlation of coronary artery atherosclerosis typing and luminal narrowing with ischemic myocardial lesions in post mortem heart specimens: a four year retrospective study. Trop J Path Micro 2018. [Google Scholar]
- N Marwah, B Sethi, S Gupta, A Duhan, S Singh, R Sen. Histomorphological spectrum of various cardiac changes in sudden death: An autopsy study. Iranian J Pathol 2011. [Google Scholar]
- SN Shah, KA Patel, HB Patel, JN Bhalodia. Histomorphological study of changes in heart - An autopsy study. Arch Cytol Histopathol Res 2019. [Google Scholar]
- S Garg, S Hasija, P Sharma, S Kalhan, N Saini, A Khan. A histopathological analysis of prevalence of various heart diseases: an autopsy study. Int J Res Med Sci 2018. [Google Scholar] [Crossref]
- C Joshi. Postmortem study of histopathological lesions of heart in cases of sudden death- an incidental finding. J Evid Based Med Healkthc 2016. [Google Scholar]
- V Porwal, S Khandelwal, D Jain, S Gupta. Histological Classification of Atherosclerosis and Correlation with Ischemic Heart Disease: A Autopsy Based Study. APALM 2016. [Google Scholar]
- M Garg, A Aggarwal, S Kataria. Coronary Atherosclerosis and Myocardial Infarction. An autopsy study. J Indian Acad Forensic Med 2011. [Google Scholar]
- R Virmani, F D Kolodgie, A P Burke, A Farb, S M Schwartz. Lessons from sudden coronary death- A comprehensive morphological classification scheme for atherosclerotic lesions. Arterioscler Thromb Vasc Biol 2000. [Google Scholar] [Crossref]
- J S Frederick, N M Richard, The Heart, V Kumar. The Heart. Robbins & Cotran Pathologic Basis of Disease: South Asia Edition. 9th Edn. 2015. [Google Scholar]
- Introduction
- Materials and Methods
- Case selection
- Exclusion criteria
- Gross examination of heart
- Microscopic examination
- Statistical analysis
- Results
- Age and sex distribution
- Weight distribution
- Clinical details
- Histopathological changes in heart
- Changes in coronary arteries
- Pattern and distribution of IHD
- Discussion
- Conclusion
- Conflict of Interest
- Source of Funding