
Introduction
SRCs have cytoplasmic large round-oval vacuole/aggregates of vacuoles pushing and compressing the nucleus to periphery. Vacuoles may contain mucin/other material/may be empty.1 Few cases have been reported previously, as seen in association with non-neoplastic/neoplastic cervical lesions, metastatic deposits or as artifactual. So due to diagnostic dilemma and rarity of such cases being reported, we present the case along with literature review.
Cass Report
A 50 years postmenopausal female presented with itching and foul smelling discharge per vaginum and no history of IUD. Local examination showed white discharge along with inflammation. Ultrasound showed 15×16mm uterine fibroid. Cytology revealed mainly benign superficial and intermediate squamous epithelial cells and interspersed SRCs, along with neutrophils. (Figure 1, Figure 2). There were other cells with single or multiple varying size vacuoles displacing nucleus. (Figure 3, Figure 4). Additional workups, colposcopy showed no abnormalities. In last 1year follow-up, she has developed no new signs/symptoms. Since clinico-radiological correlation ruled out malignancy and with no IUD history, these SRCs on cervical cytology were labelled artifactual.
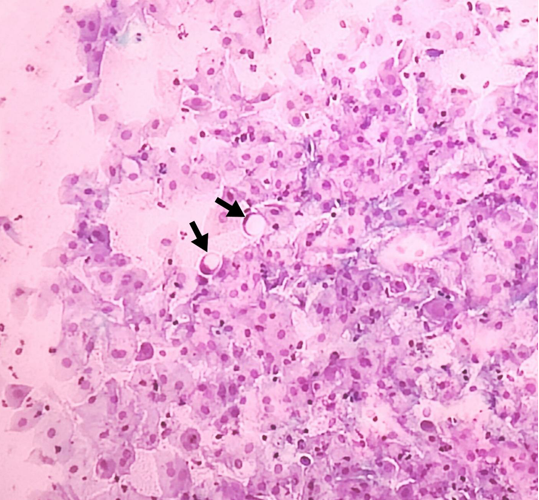
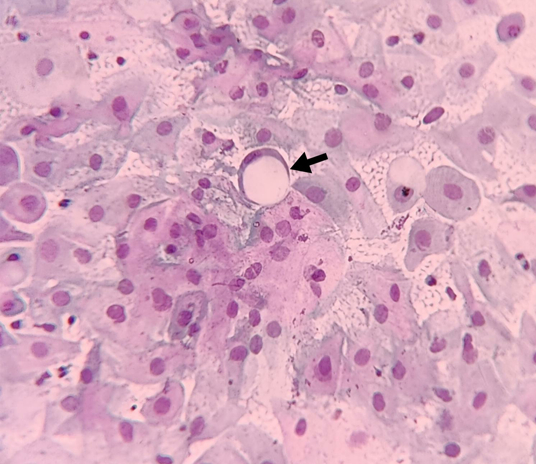
Figure 3
Cytopaslmic vacuoles seen as single large vacuole in one epithelial cell and as multiple aggregates in the adjacent epithelial cell. (Pap 1300X1100).
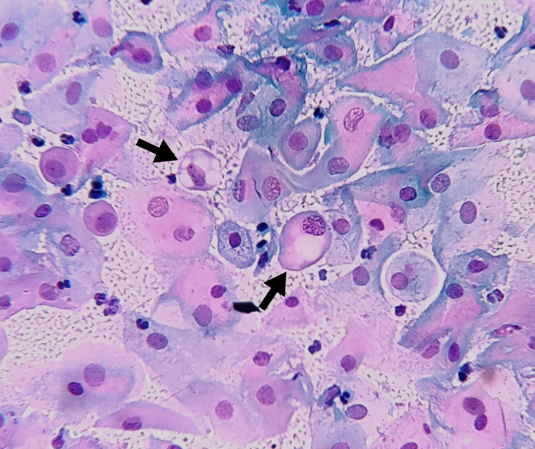
Figure 4
Multiple vacuoles forming cytoplasmic aggregates in the squamous epithelial cell which is related to artifactual changes (Pap 1200X1300).
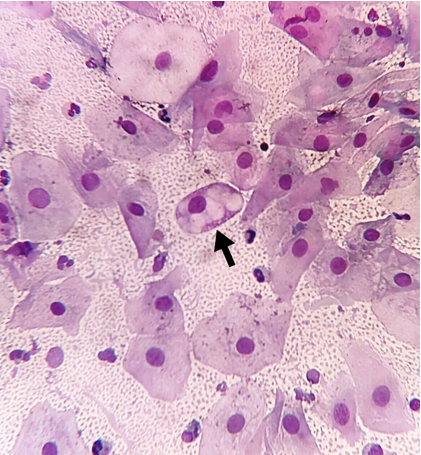
Table 1
True SRCs from false SRCs / SRLCs: Artifactual or False Signet Ring cells: Reactive-reparative cellular changes: 2, 3, 4
Table 2
Review of literature of SRCs in cervical tissues on cytology and/or histopathological examination: 5, 6, 7, 8, 9, 10
Discussion
SRCs in cervix can be seen in non-neoplastic lesions i.e. reactive-reparative, rarely in neoplasms and artifactual as seen in present case. (Table 1)2, 3, 4 Daniel F.I. Kurtycz et al documented SRCs due to chronic irritation by IUD device. With absence of other morphological features to suggest High Grade Squamous Intraepithelial Lesion (HSIL), misdiagnosis was thus avoided. Hence IUD history is important.5 There was no IUD usage in present case.
Malignancy associated SRCs, were seen on histopathology in SRC predominant cervical adenocarcinoma in a 40years female on histopathology by Kohei Hamada et al and SRC type adenocarcinoma with HPV positive full genome in a 40years female on cervical cytology by Satoshi Kawai et al.6, 7 There were supportive clinico-radiological findings like cervical mass in 48years with large pelvic mass in lower uterine segment/cervix and in 64years females with primary signet ring cell (PSRCC) carcinoma on pan hysterectomy and endometrial/endocervical curettage, diagnosed by Bernadette Cracchiolo et al and Veysel Sal et al respectively.8, 9 Correlation with clinico-radiological features is important to support the carcinoma diagnosis even after the presence of SRCs on microscopy. In the present case, no such pointers suggested suspicion towards malignancy. Various studies where morphological SRCs were found in cervix are tabulated in Table 2 along with histological diagnosis.
Cases of artifactual SRCs were reported from other sites like on duodenal (strictured area) biopsy in 89years male reported by Mark Li-chang Wu. This was at first misinterpreted as SRC carcinoma. Other indicators of malignancy were ruled out. SRCs found were detached, degenerated epithelial cells from normal glands post-procedural mechanical trauma. As proposed by author, formation of soapy water bubbles from a child's toy can be analogous for artifactual SRCs production. The cell is pushed out of gland like soapy-water film bulging out from ring, when gland being assumed analogous to plastic ring, epithelial cells to soapy-water film bound by ring and procedural trauma to airflow directed through ring. After detachment from gland (ring), cells achieve spherical shape (bubbles) to achieve physical equilibrium. They arbitrarily categorised SRCs into true and false SRCs/ SRLCs (Signet ring like cells).2
Careful microscopic examination as well as clinico-radiological correlation must be done to rule out artifactual causes of SRCs, before labelling patient as case of PSRCC carcinoma.[Table 2] 5, 6, 7, 8, 9, 10