- Visibility 30 Views
- Downloads 8 Downloads
- DOI 10.18231/j.achr.2024.040
-
CrossMark

Anaplastic carcinoma of thyroid with giant cells –Cytodiagnosis of category VI high grade thyroid tumor
- Author Details:
-
 Dhiraj B Nikumbh *
Dhiraj B Nikumbh *
High grade or undifferentiated thyroid carcinoma are uncommon findings in routine cytopathology practice. They constitute 5 to 10% all thyroid tumors. [1] Diagnostic role, sensitivity and specificity of the FNA in thyroid lesions are proven facts. It has many advantages as lines of treatment are decided on the diagnosis as per the Bethesda thyroid reporting system. There are only handful numbers of cases of anaplastic thyroid carcinoma with giant cells diagnosed on cytology. [1] Because of its challenging diagnosis with varied differential diagnosis and different treatment guidelines, provokes to write editorial on this rare terminology diagnosed on cytopathology.
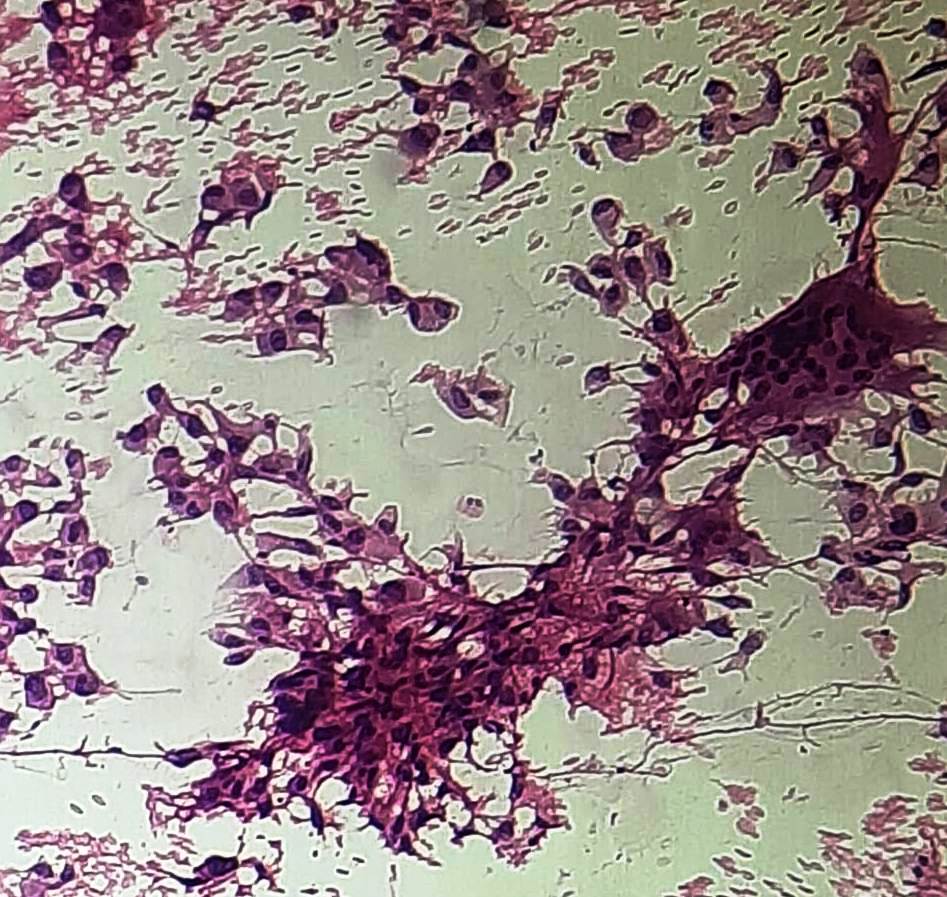
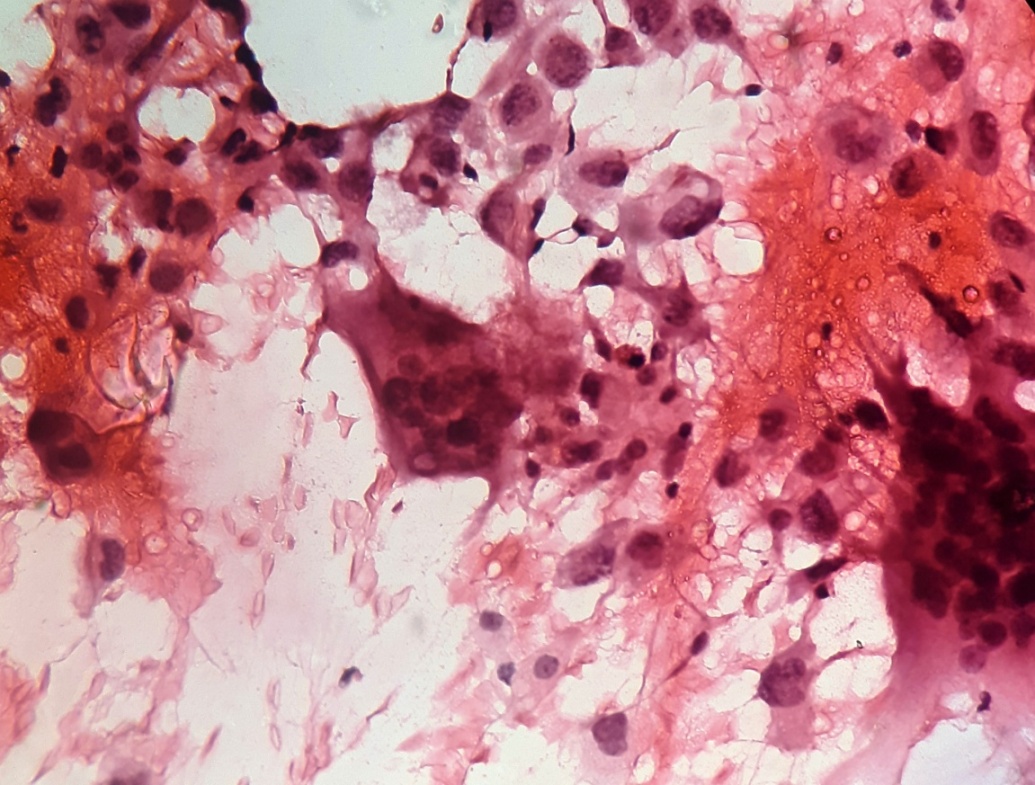
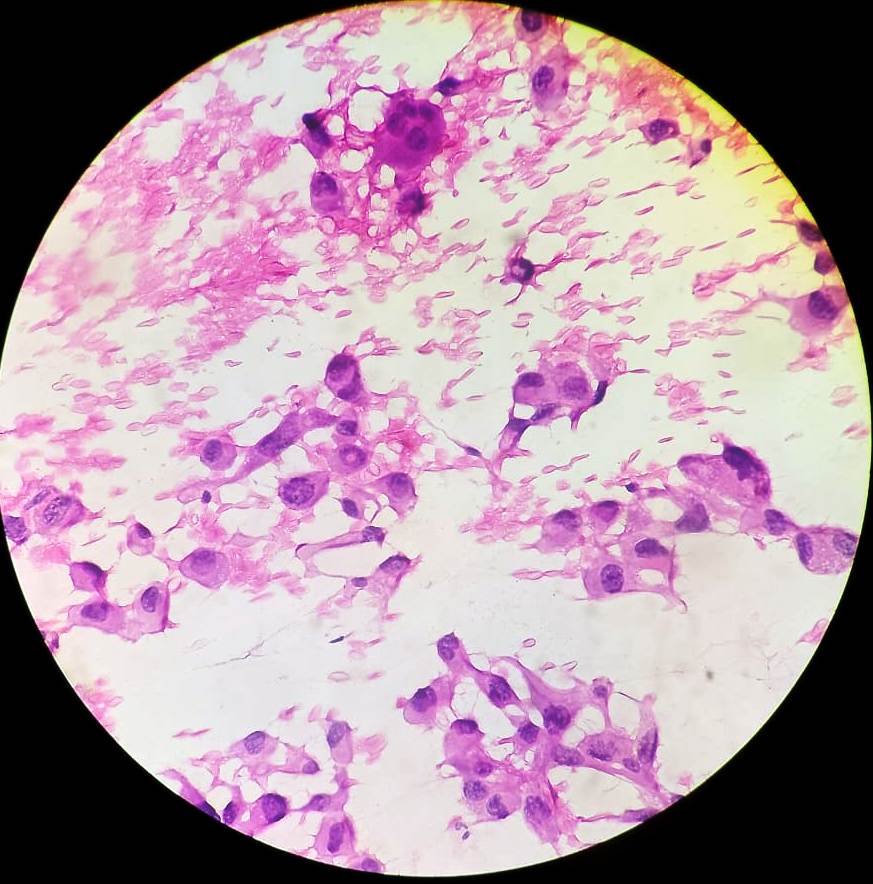
We encountered a 69 yrs old female presented to Surgery OPD department with large mass in midline neck since 3 years. The lump measures 6x5 cms and it moves with deglutition and not with protrusion of tongue. Past history of similar complaints but no treatment was taken. Surgeon advised FNA of the lump. We had done the FNAC by using 23 gauze needle under all precautions. The smears studied show sheets, microfollicles and aggregates of neoplastic thyroid follicular cells admixed with numerous multinucleated giant cells ([Figure 1]). Individual neoplastic cells are large with pleomorphic nuclei having irregular nuclear chromatin and occasional prominent nucleoli ([Figure 2]). Few of the malignant cells show intranuclear inclusions with prominent nucleoli ([Figure 3]). Background showed many multinucleated giant cells with moderate amount of dense cytoplasm admixed with scant colloid material and blood. Final Cytological impression was given as – (The Bethesda system of reporting thyroid cytopathology –Category VI Malignant.) Positive for malignant cells – s/o Anaplastic thyroid carcinoma, Giant cell variant. We lost the follow up of this patient as referred to higher center so cytohistopathological correlation was not possible.
In the existing literature and pub med data only handful, odd number of cases was reported on cytopathology of this lesion. Anaplastic thyroid carcinoma with giant cells variant is a rare entity and diagnosed meticulously as grave prognosis. There are three variants of anaplastic thyroid carcinoma as spindle cell variant, squamoid cells and giant cells varients.[1] Cytologically these patterns may be seen in combination or rarely as the isolated pattern as in our case. Anaplastic cell carcinoma with multinucleated giant cells is an uncommon lesion. This lesion categorized as per the Bethedsa system of thyroid reporting in Category VI. The giant cells in this lesion look like osteoclastic cells so many authors cite this entity as anaplastic thyroid carcinoma with osteoclastic giant cells. It encountered rarely in the routine clinical practice. [2], [3]
Anaplastic thyroid carcinoma are rapidly growing malignant tumor of thyroid affecting mainly in old age group peoples. Cytologically two cell population is diagnostic as well as problematic in diagnosis as undifferentiated mononuclear cells and osteoclastic multinucleated giant cells. [1] The neoplastic component is pleomorphic mononuclear cells and benign or reactive component is osteoclastic giant cells. [1], [2], [3]
Due to many multinucleated giant cells seen in the FNA samples of thyroid many differential diagnoses were aroused as Hashomoto’s thyroiditis, anaplastic carcinoma, papillary carcinoma, and granulomatous thyroiditis or Langerhan’s cell histiocytosis. Cytologically, reporting pathologist can differentiates these lesions on morphological features. [1], [2], [3]
Anaplastic thyroid carcinoma with giant cells often diagnosed in terminal stages as patients presented with advanced metastasis at the time of diagnosis. Hence FNA has a pivotal role in final diagnosis without invasive techniques and patient should refer to palliative chemotherapy as in our case.
In the conclusion, surgeons and pathologist should be keen to diagnose such rare lesions and uncommon high grade tumors as treatment options are limited in such setups for the old age patients. Role of FNAC is highlighted in this editorial as its uncommon nature and rarely encountered tumor in clinical practice.
Conflict of Interest
None.
References
- Dong Hoon Kang Min Han, Wonae Kim, Lee. Aspiration Cytology of the Osteoclastic Variant of Anaplastic Thyroid Carcinoma: with Special Emphasis on the Undifferentiated Mononuclear Cells. Korean J Pathol 2010. [Google Scholar]
- JH Esmaili, GR Hafez, TF Warner. Anaplastic carcinoma of the thyroid with osteoclast-like giant cells. Cancer 1983. [Google Scholar]
- MJ Gaffey, EE Lack, ML Christ, LM Weiss. Anaplastic thyroid carcinoma with osteoclast-like giant cells: a clinicopathologic, immunohistochemical, and ultrastructural study. Am J Surg Pathol 1991. [Google Scholar]