
Introduction
Myelomeningocele can occur throughout the spinal axis but the area with the least common localization is the thoracic region which is uncommon. Rarely, these abnormalities coexist with a teratoma and only few reports of a teratoma arising from a myelomeningocele have been reported.1 Myelomeningocele, part of the Neural Tube Defect (NTD) spectrum, can also be associated with some disastrous events such as paraplegia, bladder and bowel incontinence, Chiari malformation Type II, and hydrocephalus. 2 Teratomas have been considered the most common type of congenital tumours in the dorsal midline area, arising from displaced germ cells, and by definition contain ectodermal, mesodermal, and endodermal tissues. 3, 4, 5 Teratoma can also undergo malignant transformation to a non-germ cell malignancy. 2 The hypotheses of a possible common association include a single dysembryogenic process and neoplastic transformation of heterotopic primordial elements incorporated in the defect. 6, 7, 8 Here, we report an interesting case of a teratoma arising within thoracic myelomeningocele in an infant.
Case Presentation
Clinical summary
A three month old girl born via vaginal delivery to two related Fulani parents presenting with upper back swelling noticed since birth. Pregnancy was claimed to be uneventful, mother never attended any antenatal clinic and delivery was at home. On examination patient was mildly dehydrated and malnourished. Status localis revealed an intact cystic midline upper back swelling measuring about 6x4cm, non-tender with no differential warmth. Radiographic evaluation was not done due to financial constraint
Pathologic findings
Macroscopy
Three irregularly shaped firm to cystic to flabby tissues aggregating to 5x4x1.5cm, weighing 6g were received. The tissues were labeled as A, B and C. Specimen A an ellipsoid skin covered tissue with a dome shaped lesion on its surface. Specimen A measured 4.5x2.5x2cm and the dome shaped lesion measured 3.5cm in its longest diameter and 2cm above the skin surface. Specimen A weighed 5g and cut sections felt hard. Specimen B was an irregularly shaped cystic to flabby tissue measuring 4.5x2.5x0.5cm and weighed 4g. Transection through specimen B showed white homogenous areas. Specimen C was an irregularly shaped tissue measuring 3.5x3x1.5cm and weighed 2g. Transection through specimen C revealed white to brown homogeneous areas.
Microscopy
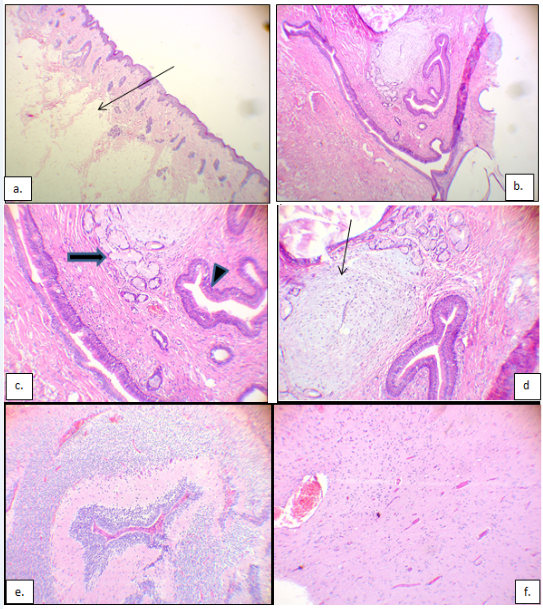
Specimen A showed a pigmented epidermis exhibiting varying degree of hyperkeratosis and atrophy with focal ulceration. This overlies a thinned out dermis and haphazard lobules of mature adipocytes almost abutting the epithelium. A focus deep within the reticular dermis showed a lesion composed of chondroid matrix, respiratory type epithelia, seromucinous glands with some few dilated forms. Areas showing skin adnexal structures were also noted. Specimen B showed fibrocollagenous tissues while specimen C showed neural tissue. (Figure 1a-f) shows the microscopic features
Figure 1
a): H&E stained photomicrograph at x40 showing epidermis, thin dermis and subcutis. Arrow showing the mature adipocytes close to epithelium; (b): H&E stained photomicrograph at x40 showing the reticular dermis having a mature teratoma composed of chondroid matrix, respiratory epithelia and seromucinous glands; (c): H&E stained photomicrograph at x100 with arrowhead and arrow showing respiratory epithelia and seromucinous glands respectively; (d): H&E stained photomicrograph at x100 with arrow showing the chondroid matrix; (e)&(f): H&E stained photomicrographs at x100 showing different fields of neural tissue in myelomeningocele.
Discussion
A dorsal midline mass in newborn may suggest a variety of diagnoses, including different types of neural tube defect (NTDs), the most common being a myelomeningocele as well as some less prevalent diagnoses such as teratoma, hamartomas or human tail. Teratoma presenting as a dorsal mass has been shown to be very rare, accounting for only 3% to 9% of all intra-spinal tumours in childhood. 1 Teratoma is a germ cell neoplasm that contains differentiated elements derived from all three germ layers. 2 This occurrence of a mature midline teratoma within a myelomeningocele in this index case is rare and what makes it even rarer is occurrence in the thoracic region which is uncommon. There are only a few published reports of coexisting myelomeningocele and intradural or extradural teratomas. 1, 9 To our knowledge few cases of thoracic myelomeningocele have been reported,.3 with an incidence of 1 per 1,000 live births as reported by Filston et al.10 Teratomas occurring independently in the absence of a myelomeningocele are much rarer with an incidence of 1 per 13,000 live births as reported by Humphreys et al.11 It is important to do a thorough clinical, radiological, and histological evaluation in order to establish the correct diagnosis. Radiologic evaluations such as Magnetic Resonance Imaging (MRI) could have been helpful in making a definite diagnosis, but because of the financial constraint faced by parents of the patient, it was not possible. Histologic evaluation still remains the main stay in the diagnosis of such conditions.
Conclusion
Myelomeningocele has variable prognosis based on localization and other accompanying abnormalities. Due to the risk of malignant transformation to non-germ cell tumours in teratoma, prompt histologic diagnosis and complete resection is important regardless of size of lesion and age of patient.